This is an automatically translated article.
The article was written by MSc Vu Ngoc Thang - Urology Surgeon, Vinmec Times City International General Hospital.Kidney cancer includes renal cell cancer, renal sarcoma and primary renal lymphoma... in which Renal Cell Carcinoma (RCC) accounts for more than 90% of cases, so in this article only Refers to the content of renal cell cancer. Renal cell carcinoma ranks second in malignancies of the urinary system and accounts for 1-2% of all cancers in adults. It usually occurs in adults over the age of 40, with twice as many men as women.
1. Causes and mechanisms of pathogenesis
Kidney tumor is initially in the parenchyma, the tumor gradually enlarges, breaks the renal capsule and spreads out to the fatty layer around the kidney, invading organs such as the colon and liver.
Renal cell carcinoma metastasizes by lymphatic and venous routes. By lymphatic route, renal cell cancer metastasizes to lumbar lymph nodes, aorta, then to retroperitoneal, abdominal, mediastinal... sometimes to supraclavicular, axillary, and cervical lymph nodes. Intravenously, the tumor metastasized to the vena cava, then to the retroperitoneal lymph nodes of the abdomen, the mediastinum and further into distant organs such as lung, liver, bone, adrenal gland, contralateral kidney, brain..
Causes, The pathogenesis of the disease is still unknown so far. However, several factors are thought to influence the occurrence of the disease.
Smoking is a risk factor for kidney cancer, about 30% of men and about 24% of female smokers get kidney cancer. The longer you smoke and the more cigarettes you smoke, the higher your risk.
Many toxins found in cigarette smoke can damage the DNA of cells, of which benzo(a)pyrene is said to damage the p53 gene - a gene that codes for proteins p53 is a protein that plays a role in protecting the body's cells against cancer
Polycyclic aromatic hydrogen carbides such as 3' - 5' benzo - pyrene have also been implicated in the occurrence of kidney cancer. Many studies show that workers in some industries exposed to polycyclic aromatic hydrogen carbides such as 3' - 5' benzo - pyrene have a high incidence of diseases such as printing, chemical, dyeing or petroleum exposure.
Genetic factors: the disease can appear in many people in the same family. People with a deletion in chromosome 3 or a translocation of chromosomes 3 and 8 also have a high incidence.
2. Pathology
2.1 Macroscopic tumor usually originates from the renal cortex, then can invade the renal calyces, invade, and break the renal cortex into surrounding organizations. The tumor section is usually dark or light yellow, alternating with necrosis, bleeding or calcification, enveloped, and proliferating blood vessels.

Hình ảnh đại thể ung thư thận
2.2 Microscopic renal cell carcinoma usually arises from the proximal tubular epithelium, consisting of clusters of closely spaced cells, separated by sparse connective tissue. These cells form a cystic structure. Cells have round or polygonal shape, small nucleus, wide and bright cytoplasm containing glycogen, cholesterol, different degrees of differentiation (commonly called clear cell tumor).
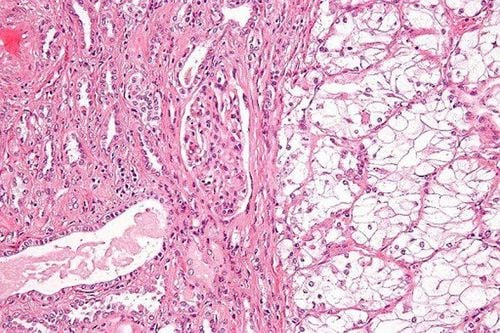
Hình ảnh vi thể ung thư thận
3. Clinical symptoms
3.1 Hematuria is a common symptom (80% of cases). Hematuria with characteristics: usually gross, whole, without blood clots, hematuria without evidence, without cause.
Some cases may have microscopic hematuria or hematuria, with blood clots, there may also be renal colic.
3.2 Low back pain With the nature of dull pain, due to the tumor growing to stretch the renal capsule. In some cases, there may be renal colic due to a blood clot blocking the urinary tract.
3.3 Feel the lumbar tumor In the case of the patient coming to the clinic late. A solid mass with irregular or rough margins may be examined, with little mobility.
Hematuria, low back pain and lumbar tumor are considered the 3 classic symptoms of kidney cancer.
3.4 Other symptoms + Can detect varicocele on the same side as renal tumor.
+ Persistent fever due to necrosis in the kidney or the thermogenic substances of renal cell carcinoma.
+ Polycythemia, accompanied by headache, fatigue, dizziness, numbness in the extremities, visual disturbances.
+ The body condition rapidly deteriorates, anorexia, weakness, anemia, low fever, erythrocyte sedimentation rate increase.
+ Liver is enlarged, smooth, painless, accompanied by increased alkaline phosphatase, decreased prothrombin ratio, decreased blood albumin (Stauffer's syndrome).
+ High blood pressure due to tumor secreting more renin or due to compression of the renal artery.
3.5 Symptoms of metastasis to other organs In the case of metastases of cancer to the lungs, liver, bones and other organs, the patient may present with symptoms of these organs.
Or conversely, cancer is discovered by accident, when there are no clinical signs, when taking venous urographs, ultrasound, CT Scanner, lung ... These cases are more and more thanks to popularity of diagnostic imaging tools.
4. Subclinical symptoms
4.1 Ultrasound This is a commonly used method, valuable because it has the ability to detect small tumors without clinical manifestations.
The image on ultrasound is an echogenic mass. Ultrasound measures the size, assesses the tumor location, invasion status and pyelonephritis morphology.
Ultrasound can detect metastases in liver, lymph nodes, thrombosis in renal vein, vena cava...
4.2 Unprepared urogram An unprepared urogram can show an irregular kidney shadow , larger than normal, may be accompanied by calcifications.
4.3 Intravenous drug nephrography (UIV) Can see amputations, sometimes shows compression, stretching, and displacement of the renal calyces.
Tumors in the lower pole of the kidney can also show compression of the ureter.
In addition, the UIV film also shows the drug secretion and circulation of each kidney.
In some cases where the renal cell carcinoma is too large, destroys most of the renal parenchyma or obstructs the renal vein, or the blood clot compresses the renal calyces, the kidneys will not secrete contrast into the renal calyces.
4.4 Computed tomography Computed tomography (CT) is the most valuable method in diagnosing kidney cancer, on computed tomography to evaluate the tumor location, size, boundary and extent of invasion. tumor invasion. In addition, computed tomography can evaluate the condition of the healthy kidney parenchyma and the contralateral kidney.
Renal cell carcinoma is often presented as a heterogeneous mass, equal in density or inferior to renal parenchyma. After contrast injection, the tumor emerged as an area of high density compared with the normal renal parenchyma in the arterial phase. Areas of necrosis are less dense.
In addition, computed tomography can also detect lymph node, liver metastases...
Multi-sequence computed tomography detects lesions more accurately than conventional CT scans, especially in invasion into the renal pelvis, blood vessels, lymph node and distant metastases.
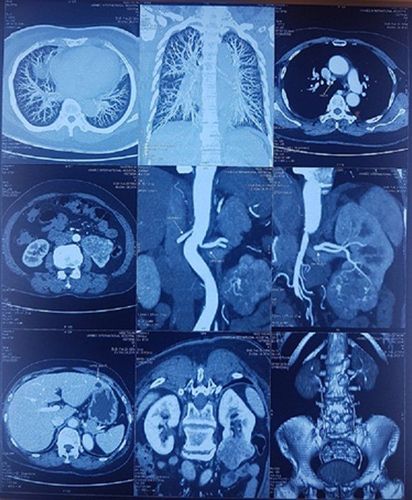
Khối u thận trái trên phim chụp cắt lớp vi tính
4.5 Renal Angiography Angiography is an important diagnostic modality for renal tumours. This method allows to see very strong perfusion, proliferative images of the arterial system and blood pools, fast venous return time, avascular imaging due to necrosis. Some renal cell cancers are poorly perfused (10% of renal cancers).
This method is a method for definitive diagnosis, important differential diagnosis for renal tumors.
Classical renal angiography is usually applied by the Seldinger method. Currently, people apply multi-section CT scan, take the film in the renal artery phase.
Renal angiography can also be combined with renal artery occlusion to facilitate surgery.
4.6 MRI On MRI film assesses tumor location, size, boundary and extent of invasion. Helps to distinguish a cyst from a solid tumor, detects blood clots in the venous system. renal vein, vena cava. 4.7 Blood tests Blood count: Usually little change Red blood cells decrease, hemoglobin decreases if hematuria persists White blood cells may increase if tumor superinfection Biochemical tests: little change. Blood calcium levels increase due to cancer secreting parathyroid hormone-like substances, or metastases to bone causing stimulation of osteoclasts to function. Some markers such as: E-Cadherin, p53, VEGF (vascular endothelial growth factor) are being studied but the specificity of these markers is not clear so far.

Xét nghiệm máu góp phần chẩn đoán ung thư thận
5. Stage division
5.1 TNM division T (tumor)
T1 Tumor size < 7cm, localized in the kidney; T2 Tumor size ≥ 7cm, localized in the kidney; T3 Tumor has spread to a large vein or infiltrates the adrenal gland or perirenal fat, but has not spread beyond the Gerota fascia; T3a Tumor invades the adrenal gland or perirenal fat, but has not invaded the Gerota fascia; T3b Tumor invades renal vein or vena cava; T4 U invades beyond the Gerota fascia. N (Nodal)
Regional lymph nodes are those located in the hilum of the kidney, around the abdominal artery and vena cava. Contrast invasion does not affect the classification criteria of N:
N0 No lymph node metastasis; N1 Metastasis to 1 regional lymph node; N2 Metastasis in more than 1 regional lymph node less than 5 cm; N3 Metastasis to more than 1 regional lymph node greater than 5 cm. M (Distant metastasis)
Mx undetermined distant metastasis; M0 No distant metastases; M1 There is distant metastasis. 5.2 Stage division
| Giai đoạn I: | T1 | N0 | M0 |
| Giai đoạn III: | T1 | N1 | M0 |
| Giai đoạn III: | T1 | N1 | M0 |
| T2 | N1 | M0 | |
| T3a | N0, N1 | M0 | |
| T3b | N0, N1 | M0 | |
| Giai đoạn IV: | T4 | Mọi N | M0 |
| Mọi T | N2, N3 | M0 | |
| Mọi T | Mọi N | M1 |
5.3. Staging according to Robson Stage I: Tumor is localized in renal parenchyma.
Stage II: Tumor is localized in the fatty layer around the kidney.
Stage IIIA: Tumor invades renal vein.
Stage IIIB: Tumor invades nearby lymph nodes.
Stage IIIC: Tumor invades both nearby lymph nodes and renal vein.
Stage IVA: Tumor invades nearby organs.
Stage IVB: There have been distant metastases.
6. Diagnosis
6.1 Confirmative diagnosis based on Clinical:
Low back pain. Peeing blood for no reason. Lumbar tumor. Subclinical:
Ultrasound: abnormal echogenic mass in renal parenchyma. X-ray: On computed tomography, the mass is increased or less dense compared to the renal parenchyma. 6.2 Differential diagnosis from 6.2.1 Other tumors in the kidney Teratoma: within the tumor there is a contrast image of bone, teeth... Renal lipoma has faint areas due to fat in the tumor. . Renal calyx carcinoma. Renal sarcoma Enlarged kidneys due to other causes: enlarged kidney due to stones, polycystic kidney... Renal cysts Inflammatory masses: renal abscess, pus-filled kidney, renal tuberculosis.... Tumors of neighboring organs Liver tumors, tumors adrenal gland, colon tumor, ovarian cyst
7. Treatment
7.1 Surgical treatment 7.1.1 Radical nephrectomy Indications: Radical nephrectomy is applied to cases of stage IIIA renal cell cancer according to Robson's staging.
Technique: Radical nephrectomy includes total nephrectomy with adjacent lymph node removal, adrenalectomy, perirenal fat removal, ovarian vasectomy or spermatic cord vasectomy, hematopoiesis. Venous block if present. This is the classic method. Currently, the concept of radical nephrectomy has changed: the adrenal gland is only removed when the tumor invades through the cortex upward.
Surgical method: open surgery, laparoscopic surgery, or robot surgery depending on the stage of the disease, the hospital's equipment and the surgeon's qualifications.
Currently, robot surgery is the most advantageous and safest method to operate on patients due to the flexibility of the robot arm, 3D rendering of the surgical area, and less damage to neighboring organizations. ..

Hình ảnh cắt thận toàn bộ do ung thư
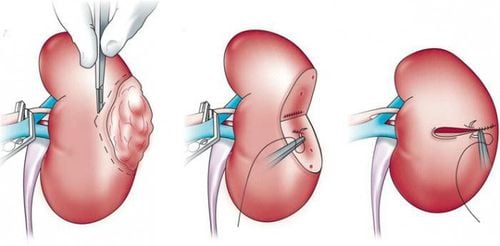
7.1.2 Partial nephrectomy Indications:
Apply in case the tumor is limited to only 1 pole of the renal parenchyma.
The tumor is smaller than 4cm, located far from the renal peduncle and the surgeon's qualifications allow it.
Technique: Can cut wedges or flat circles, cut all tumor tissue to 1cm healthy tissue, cold biopsy the section to ensure all cancer tissue.
Surgical method: Open surgery, laparoscopic surgery or Robot surgery. In which, Robotic surgery is currently the most advantageous and safest method to operate on patients.

Hình ảnh cắt thận bán phần bằng Robot
7.1.3 Nephrectomy Applied in cases of advanced cancer to remove tumor and necrotic tissue, treat prolonged hematuria...
7.2 Radiotherapy Preoperative radiotherapy The aim is to reduce bleeding Radiation therapy after nephrectomy to kill any remaining cancer cells Irradiation dose from 20 to 40 Gy depending on the location of metastases 7.3 Chemotherapy Kidney cancer is one of the diseases The strongest drug-resistant malignancy, so there is no specific chemotherapy for kidney cancer. Currently, only common chemicals such as Vinblastine are used, which is one of the most frequently mentioned chemotherapy agents for kidney cancer, but only 15-20% of patients respond well. Some other chemicals against kidney cancer have been used, but so far have not been highly effective such as Zalcitabine, Fluorouracil.
7.4 Other methods 7.4.1 Immunotherapy Designed to boost the body's natural immunity against cancer cells.
Many authors are now using Cytokines such as Interferon, Interleukin, Glutathione... for treatment with good effect but the drug price is still very expensive.
7.4.2 hormone Some authors use progesterone, androgen, antiestrogen for treatment, but the effect is not clear
7.4.3 Renal artery occlusion Relieves symptoms in inoperable patients . The goal is to limit the source of nutrients for the tumor. Some cases are applied before partial nephrectomy
7.4.4 Targeted drugs Some drugs such as Sunitinib (Sutent), Sorafenib (Nexavar), Pazopanib (Votrient).... help prolong the time. live longer and relieve symptoms for patients.
7.4.5 Physical Methods Radiofrequency Intervention (RFA): Is using a needle to poke the tumor, destroy malignant cells with ultrasound waves.
Cryotherapy: freezing cancer cells into the tumor tissue through a small incision through positioning by CT or cell cryotherapy.

Phẫu thuật nội soi với Robot hỗ trợ được thực hiện tại Bệnh viện Đa khoa Quốc tế Vinmec
Department of Urology at Vinmec has successfully performed many laparoscopic and open surgeries to treat emergency diseases of gastrointestinal - hepatobiliary; orthopedic; Urological surgery... The hospital is equipped with modern and advanced machinery such as: gastrointestinal endoscopic surgery machine, C-ARM, arthroscopic surgery machine to help support doctors in the process. surgical procedure.
Minimally invasive laparoscopic surgery with Robot supports maximum removal of cancerous tissue with minimal invasion, patients have less pain, less blood loss, fast recovery, shorten hospital stay. Laparoscopic surgery with Robot is one of the modern and effective surgical methods in the treatment of kidney cancer.
Laparoscopic nephrectomy or partial nephrectomy with handheld robot is being performed at Vinmec International General Hospital. With modern equipment system and international standard operating room. The Dex Flex Robotic Arm is one of the most advanced, sophisticated, state-of-the-art vehicles.
Customers can directly go to Vinmec Health system nationwide to visit or contact the hotline here for support.
Reference article:
European Association of Urology 2018 Kidney Cancer, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. Smith' General Urology - Fourteenth Edition- A Simon & Schuster Company. 2010 Campbell SC, Novick AC, Belldegrun A et al: Guideline for management of the clinical T1 renal mass. J Urol 2009; 182: 1271. Guideline for Management of the Clinical Stage 1 Renal Mass. American Urological Association 2009. MORE:
In what cases is partial nephrectomy indicated? Advantages of laparoscopic nephrectomy in the treatment of kidney diseases Advances in the treatment of kidney cancer