This is an automatically translated article.
Sodium is an important electrolyte, demonstrating the function of cell membranes. When hyponatremia occurs, electrical activity is easily affected, causing serious consequences. However, if the syndrome is due to abnormal ADH secretion, the core treatment of hyponatremia is simply to limit fluid intake rather than replace hypertonic sodium.
1. What is the syndrome of abnormal ADH secretion?
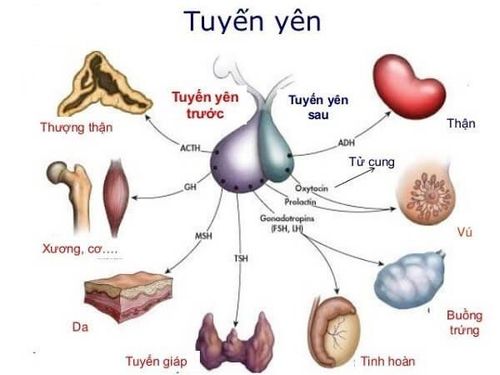
Syndrome of abnormal ADH secretion or syndrome of inappropriate antidiuretic hormone secretion (SIADH) is associated with continued excessive secretion of vasopressin (ADH) into the circulation despite normal or increased plasma volume. .Under the effect of the amount of ADH, the amount of water in the circulating volume is limited to excrete out, that is, there is an increase in water retention and thus hyponatremia. Hyponatremia is defined as a serum sodium concentration below 135 mmol/L. However, hyponatremia in the syndrome of abnormal ADH secretion will be accompanied by a concomitant decrease in serum osmolality (serum osmolality below 280 mOsm/kg. In contrast, urine osmolality is less than 280 mOsm/kg. However, it should be noted that the difference between hyponatremia due to syndrome of abnormal ADH secretion and hyponatremia in other etiologies is due to the consequence. of excess water, increased blood dilution instead of sodium deficiency.

Hội chứng bài tiết hormone chống bài niệu không phù hợp
2. What are the signs and symptoms of abnormal ADH secretion syndrome?
Depending on the extent and rate of disease progression, hyponatremia may or may not cause symptoms. At the same time, the signs of acute hyponatremia in the syndrome of abnormal ADH secretion are sometimes not exactly correlated with the severity of the hyponatremia.
Accordingly, the symptoms of hyponatremia in the syndrome of abnormal ADH secretion may have the following manifestations:
Decreased level of consciousness, confusion, disorientation, delirium, Overall muscle weakness, weakness muscle tremors, heart rhythm disturbances, arrhythmias, dysrhythmias, Cheyne-Stokes respiratory patterns, generalized convulsions, coma In addition to the above-mentioned signs, the patient also has manifestations of the underlying cause presenting with syndromes of abnormal ADH secretion, such as severe infection or extensive brain damage.

Người bệnh rơi vào trạng thái hôn mê
3. How is abnormal ADH secretion syndrome diagnosed?
In the absence of a quantitative blood test for ADH levels, the only way to confirm the diagnosis of ADH syndrome is best defined by the classical Bartter-Schwartz criteria, which can be summarized as follows:
Hyponatremia with commensurate hypotension Kidneys continue to excrete sodium in the urine Low urine volume and high electrolyte concentrations No clinical evidence of volume depletion Impossible to resolve Investigate other causes of hyponatremia Hyponatremia can be corrected only by fluid restriction In addition, the following laboratory tests may also aid in the diagnosis of a syndrome of abnormal ADH secretion:
Quantification of serum sodium concentration and associated potassium, chloride and bicarbonate measurement of plasma osmolality Measurement of urine osmolality Quantification of blood nitrogen and creatinine levels Quantification of blood glucose Quantification of serum uric acid levels Quantification of serum uric acid levels Blood cortisol Quantification of thyroid-stimulating hormone (TSH) Quantitative concentration Plasma ADH

Một số xét nghiệm giúp chẩn đoán bệnh lý
Imaging studies may be considered in ADH syndrome such as chest x-ray to detect an underlying pulmonary pathological cause of ADH syndrome.
In addition, computed tomography or magnetic resonance imaging of the brain is used to detect cerebral edema complications due to the syndrome of hypersecretion of ADH. From there, the clinician can know whether the patient's central nervous system dysfunction is caused by hyponatremia causing ADH syndrome or the etiology is lesions from the brain. Simultaneously, concurrent cranial imaging in this setting helps to rule out other potential causes that may also be responsible for the altered neurologic status.
4. How to correct hyponatremia due to abnormal ADH secretion syndrome
Treatment of the syndrome of abnormal ADH secretion mainly revolves around correcting hyponatremia. This adjustment depends on the degree of hyponatremia, whether the patient is symptomatic, and whether the condition is acute (less than 48 hours) or chronic. Measurement of urine osmolality and creatinine clearance must also be considered when choosing a treatment regimen.
Of these, treatment for hypernatremia should be indicated in patients with severe symptoms (eg, convulsions, dizziness, coma, and respiratory arrest), regardless of the degree of hyponatremia.
Hyponatremia in the setting of abnormal hypersecretion of ADH should be carefully corrected instead of sodium replacement alone. Correcting hyponatremia too quickly can lead to central pontine breakdown and consequent permanent neurological damage. It is important to remember that even severe hyponatremia can be corrected rapidly by limiting fluid intake without the need for hypertonic sodium infusion.
Thus, the goal of correcting hyponatremia at a rate that does not cause neurologic complications is to increase serum sodium levels by 0.5-1 mEq/hour and not to exceed 10-12 mEq in the first 24 hours, aiming for to a maximum serum sodium of 125-130 mEq/L.

Bệnh nhân có triệu chứng co giật cần điều trị tăng natri máu
The following are specific guidelines for managing serum sodium in ADH:
Limiting fluid intake is a first-line treatment. If serum sodium has not improved, the next treatment is increased oral sodium intake in combination with a low-dose loop diuretic. Consider treatment with hypertonic sodium infusion if serum sodium levels are not corrected after 24-48 hours of water restriction or if the patient excretes urine containing high sodium concentrations. If the above methods do not work, consider a Vasopressin-2 receptor antagonist (conivaptan or tolvaptan), which will not require fluid restriction at this time. Concomitantly, lithium receptor antagonists, demeclocycline, or vasopressin should not be used in the correction of hyponatremia in the syndrome of abnormal ADH secretion. The syndrome of hypersecretion of ADH is a progressive consequence of serious diseases in the body that cause hyponatremia. However, today, when medicine has developed greatly, patients with severe disease will be screened for the possibility of hyponatremia due to abnormal ADH secretion syndrome, thereby making an accurate treatment plan. , improve disease prognosis.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.
Customers can directly go to Vinmec Health system nationwide to visit or contact the hotline here for support.
MORE:
How to calculate creatinine clearance coefficient What role does ADH play? TSH hormone and its significance in the screening diagnosis of thyroid diseases