This is an automatically translated article.
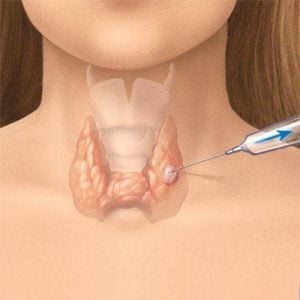
Posted by Doctor Bui Thi Hong Khang - Laboratory Department - Vinmec Central Park International General HospitalFine needle aspiration (FNA) is the most widely used diagnostic tool for breast cytology in the world. FNA is useful because it is a simple, quick, inexpensive, low-complicated diagnostic technique with high accuracy (sensitivity 80-100%, specificity over 99%).
1. Introduction
Breast cytology includes Nipple Secretion Cytology and Fine Needle Aspiration Cytology (FNA).
Nipple discharge outside of pregnancy or lactation is an unusual symptom, possibly due to a physical lesion in the breast (eg, intraductal papilloma or cancer) or an endocrine abnormality (eg, pituitary tumor causing increased prolactin secretion). Nipple secretions are often poor in cells, and only a small percentage of patients have symptoms of nipple discharge, so cytology of nipple discharge is of little value in the diagnosis of mammary gland diseases and screening. breast cancer. Investigation of nipple discharge is usually indicated only in cases of abnormal discharge but no palpable or visible lesions on mammography and ultrasound. Fine needle aspiration (FNA) is the most widely used diagnostic tool for breast cytology in the world. FNA is useful because it is a simple, quick, inexpensive, low-complicated diagnostic technique with high accuracy (sensitivity 80-100%, specificity over 99%). To get the most accurate diagnosis, it is necessary to compare the clinical examination, imaging (mammography/ultrasound) and FNA. In the presence of incompatibility of any of the three factors above, additional diagnostic methods must be performed (such as core needle biopsy or open biopsy). Indications for breast FNA include: Palpable breast lesions; lesions are not palpable but can be seen by ultrasound/mammography; the breast wrap; lesions suspected of recurrence.
Tăng sinh kèm không điển hình tế bào được xếp vào nhóm 3
2. Fine needle aspiration cytology of mammary gland lesions
2.1 Results response system
Standardization of cytology results makes it easier for clinicians to decide on the next course of treatment for a patient. The cytological findings are usually classified into 5 groups as shown in the following table.
Group 1 - does not meet diagnostic criteria:
When the smear has too few epithelial cells; the smear is too thick, the cells are covered by red blood cells; or cells are not well preserved (crushed, poorly fixed). The diagnostic criteria are met when on 2 slides there are at least 6 clusters, each cluster of 15 epithelial cells.
Group 2 - benign:
When the smear meets the diagnostic criteria and has no malignant features. This group includes benign lesions such as inflammation, fat necrosis, fibrous changes, encapsulation, fibroadenoma, etc. However, it is not always possible to diagnose each disease entity separately.
Group 3 - atypical/significance undetermined:
When the smear has a benign image but some additional benign atypical features such as sporadic cells, some cells have slightly nuclei big and distorted. Some smears with papillary or mucoid structures are also included in this group.
Group 4 - suspected malignancy:
When the smear has features that are indicative but not sufficient for a diagnosis of malignancy. For example, malignant cells are evident but too few or obscured; or cells with atypical nuclear status worse than group 3 but not enough to be classified in group 5.
Group 5 - malignancy:
When smear has clear malignancy. Determine whether the malignant lesion is carcinoma, sarcoma, or lymphoma. For breast carcinoma, it is possible to refer to some specific histological types, such as lobular infiltrative carcinoma, mucinous, ductal carcinoma, ..
2.2 Mastitis:
Inflammation of the mammary gland is rare, including many types: acute inflammation, chronic inflammation, granulitis; due to various causes such as infection, trauma or unknown cause. FNA can confirm the diagnosis of inflammatory lesions, avoid surgery, and also serve as a contributing modality to treatment (eg, purulent aspiration in acute abscessed mastitis).
2.3 Lactating adenoma and breast tissue changes due to lactation
FNA is more useful than other means in the diagnosis of breast lesions during pregnancy and lactation because the patient does not radiation exposure due to mammography or anesthetics due to biopsy.
3. Fibrocystic changes
The most common lesion (50-90% of adult women), associated with hormone imbalance (excessive estrogen or progesterone deficiency). The primary lesion patterns of fibrous alterations are encapsulation and fibrosis, with or without varying degrees of epithelial hyperplasia. In some cases, sheath changes may increase the risk of breast cancer. Benign capsule completely collapsed after aspiration. Occasionally a malignant lesion may be adjacent to and obscured by a benign fascia; Therefore, if after aspiration is still palpable a mass or a lump, this lesion should be aspirated again.
Hyperplasia with atypical cells is classified in group 3 , need to compare with clinical and imaging to consider the indications for biopsy and histopathological examination. About 1/3 of the cases of proliferation with cytologic atypia have histopathological findings as malignant lesions such as carcinoma in situ, low-grade invasive carcinoma.
4. Fibroids - epithelial
Tumors composed of two components epithelial and stromal proliferation, including fibroadenomas and phyllodes tumors.
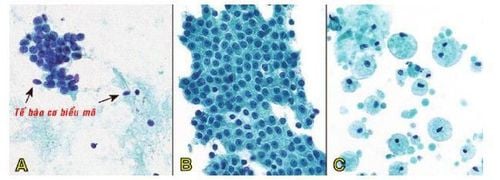
Fibroadenoma:
U sợi tuyến, tế bào biểu mô kết đám giống “sừng hươu” (A) hoặc mảng lớn hình tổ ong (B); nền phết chứa nhiều tế bào cơ biểu mô và các mảnh mô đệm dạng niêm (C).
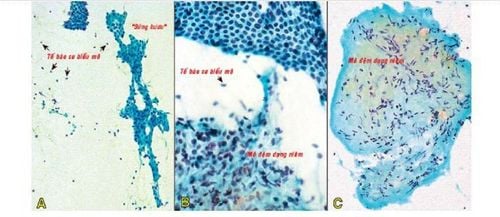
Phyllodes tumors:
Clinical features:
Phyllodes tumors only account for <1% of breast tumors. The average age of Asian patients is about 25 to 30 years old, lower than European and American patients. Lymphoma is usually a solitary mass, one breast, firm, not attached to the skin, fast growing, the average size is about 4-5cm. Tumor can reach 10 - 20cm in size, the skin on the tumor is glossy, the veins are bulging on the surface of the tumor. The majority of phyllodes tumors are benign, the rest are borderline and malignant neoplasms. The likelihood of recurrence and metastasis differs between benign, borderline and malignant tumors. Differential diagnosis with fibroadenoma should be made before surgery, because for fibroadenoma, only tumor removal is required, but for phyllodes tumor, it must be resected to avoid recurrence.
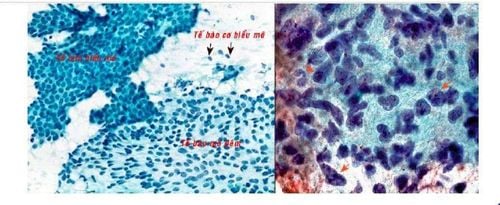
Phết tế bào của u diệp thể lành cũng gồm 2 pha giống như u sợi tuyến (so sánh với hình 8B); chỉ khác là có thành phần biểu mô tăng sinh mạnh hơn, tạo thành các mảng lớn; nhiều mảnh mô đệm giầu tế bào với các tế bào mô đệm có nhân hình thoi (A). U diệp thể ác có thành phần mô đệm tăng sinh mạnh, với nhân hình thoi lớn, tăng sác dị dạng, hạch nhân to rõ (mũi tên) (B).
5. Papillary lesions
It accounts for only a small percentage of mammary gland diseases, but is a very complex group of entities ranging from benign to malignant, and is characterized by papillary hyperplasia. Benign papillary lesions are intraductal papillomas, malignant papillary lesions include local and infiltrative papillary carcinomas. Differential diagnosis between benign and malignant papillary lesions is difficult on cytology; because in benign papillomas, atypical cells may be encountered; In contrast, in papillary carcinoma, the epithelial cells are sometimes homogenous or very slightly deformed. Thus, for a specimen rich in cells and with a network of papillary structures, the cytosolic reader can only answer papillary lesions and class 3; This result requires biopsy and histopathology to differentiate between benign and malignant.
6. Carcinoma of the breast
Breast carcinoma accounts for about 99% of malignancies of the breast, the first cancer in Vietnamese women. The peak age of the disease is 40-50 years old. Tumors can be very small, not palpable, only detectable by mammography; but usually at the time of diagnosis, the tumor is a mass about 2-3 cm in size, relatively well-defined; solid density.
In general, FNA technique has advantages of fast, accurate and low cost, but also has certain limitations. First, the smear aspiration cells no longer retain histological structural features, so the cytological diagnosis of group 5 cannot distinguish between carcinoma in situ and invasive carcinoma, which are two entities with different treatments. Therefore, with cytological diagnoses of groups 4 and 5, biopsy is required for histopathological diagnosis.
Second, with cytology results of group 3, biopsy is still required to rule out malignancy. Perhaps this is the reason why hospitals in Europe and the United States have recently tended to replace FNA with core biopsy in the diagnosis of mammary malignancy. However, FNA is still very effective in confirming the benign nature of breast lesions diagnosed through clinical and imaging studies; as well as in the diagnosis of locally recurrent lesions of breast cancer; Thus, patients do not have to biopsies, saving time and costs.
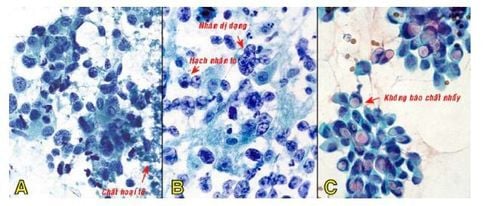
Carcinôm tuyến vú grad cao, phết giầu tế bào, kết đám lộn xộn hoặc phân bố rời rạc, tế bào đa dạng, nhân to tăng sắc, nền tiêu bản có chất hoại tử (A); một trường hợp khác, tế bào u có nhân rất dị dạng, hạch nhân to, tỉ lệ nhân/bào tương tăng (B); trong 20% trường hợp carcinôm tuyến vú, tế bào u có bào tương chứa một không bào chất nhầy giới hạn rõ (C).
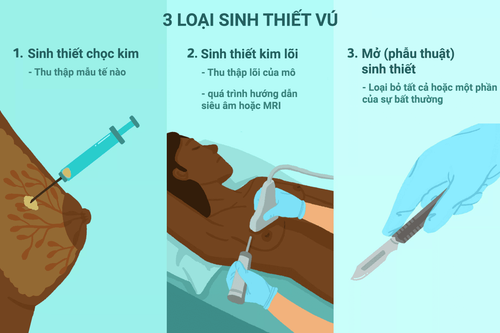
Currently, Vinmec International General Hospital is one of the very few hospitals in the country that applies the technique of breast biopsy with vacuum-assisted vacuum aspiration under Stereotactic positioning. This technique is more effective than the core needle biopsy method: Thanks to the use of a biopsy needle with a large size of 12 G or more, combined with vacuum suction, it helps to get more samples, thereby making it possible to obtain more samples. higher probability of success. In addition, this technique is also less invasive than the open biopsy method: The incision site does not require any recovery stitches, does not require special care, and the patient can return to normal daily life right away. tomorrow. In addition, the placement of markers to mark the intervention site is carried out right in the procedure to help manage the lesions after the test results are more favorable.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References: GPB Textbook GPB Department of Medical University Pham Ngoc Thach HCMC.