This is an automatically translated article.
The article is expertly consulted by Master, Doctor Ton That Quang - Head of Anesthesia - Anesthesia Unit - Department of General Surgery - Vinmec Nha Trang International General Hospital.Endoscopic interventional hysteroscopy is a modern method to help treat diseases of the uterus. This method is performed by specialists using endotracheal anesthesia.
1. Endotracheal anesthesia What is interventional hysteroscopy?
Endoscopic endotracheal anesthesia intervention is a modern technique, performed by general anesthesia with intubation. The main purpose of this technique is to control breathing during surgery and to assist in postoperative resuscitation.2. When is the indication for interventional hysteroscopy under endotracheal anesthesia?
Submucosal fibroblasts. Separation of uterine adhesions. Burn or remove polyps of the uterus (cut the polyp stalk with scissors, ring electrode or plan the polyp into small pieces with a cutting ring). Fallopian tube pump. Treatment of ectopic pregnancy. Shape the fallopian tube, reconnect the fallopian tube. Indications for endotracheal anesthesia when mask airway control is difficult. Indications for endotracheal anesthesia when maintaining anesthesia by inhalation anesthetics.
Bệnh nhân cắt polyp buồng tử cung được chỉ định nội soi buồng tử cung can thiệp
3. Contraindications for hysteroscopy with endotracheal anesthesia?
The rupture of an ectopic pregnancy causing vascular collapse does not apply laparoscopic methods. The patient did not agree to undergo general anesthesia. Medical facilities do not have enough facilities for anesthesia and resuscitation Anesthesiologists have not been trained in endotracheal anesthesia techniques.4. The person performing the anesthetic technique
Specialist doctors and nurses have been trained in general anesthesia through endotracheal tubes as well as methods of resuscitation and management of complications caused by anesthesia.5. Interventional endotracheal endotracheal anesthesia procedure
5.1 Preparation for endotracheal anesthesia
System of anesthesia machine, ventilator, oxygen source, monitor to monitor vital signs, defibrillator, suction machine... Intubation instruments such as laryngoscope, endotracheal tube size, suction tube, mask, squeeze ball, oropharyngeal cannula, Magill pliers, soft mandrin... Some drugs to support intubation: Lidocaine 10% spray, Salbutamol spray. Supportive devices for difficult intubation: Cook tube, laryngeal mask, flexible bronchoscope, tracheostomy kit, mouth opener...
Lidocain 10% dạng xịt giúp hỗ trợ đặt nội khí quản
5.2 Prepare the patient for anesthesia
Patients should have a comprehensive preoperative examination under general anesthesia to detect and prevent risks, and be explained about possible complications. Patients should be evaluated for difficult intubation and sedated the night before surgery (if necessary). Check administrative records, identify the patient's name, dentures, last meal time before the procedure. With the patient lying on his back, give oxygen through the nose at a concentration of 3-6 l/min at least 5 minutes before induction of anesthesia. Install a monitor to monitor vital signs such as pulse, blood pressure, breathing rate, SpO2 and must have EtCO2 parameters in laparoscopic surgery. Establish an intravenous line (used in emergency situations).
Bệnh nhân có thể uống thuốc an thần nếu bị kích động quá
5.3 Initiating drug anesthesia
Intravenous anesthetics (propofol, etomidate, thiopental, ketamine...) or volatile anesthetics (sevoflurane, Isoflurane..). Painkillers: fentanyl, sufentanil, morphine... Muscle relaxants (if needed): succinylcholine, rocuronium, vecuronium...5.4 Oral intubation technique
Right hand open mouth, tilt the patient's neck. The left hand holds the laryngoscope into the patient's mouth from the right side of the mouth, moves the tongue to the left and pushes the light deep in, in coordination with the right hand to press the cricoid cartilage to find the epiglottis and glottis. Then proceed to rapid induction of anesthesia. Gently insert the endotracheal tube through the glottis under the guidance of the lamp. When the balloon of the endotracheal tube passes through the vocal cords 2-3 cm, it stops. Inflate the tube insert to secure the tube in the trachea. Check that the tube position is correct in the trachea by squeezing the balloon through the endotracheal tube while listening to the bronchi, observing the patient's SpO2. When the endotracheal tube is in the correct position, gently withdraw the laryngoscope. Secure the tube with adhesive tape. Place the cannula in the patient's mouth to avoid biting the tube (if necessary). In case of difficult intubation: apply difficult intubation procedure.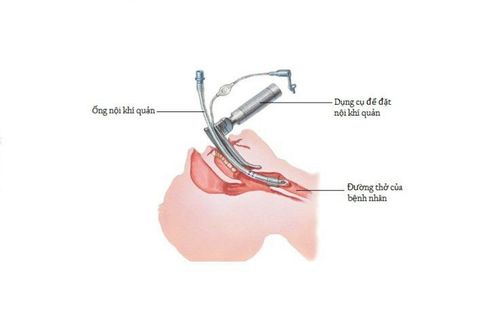
Kỹ thuật đặt nội khí quản qua đường miệng
5.5 Steps to maintain endotracheal anesthesia
Maintain anesthesia during interventional laparoscopic surgery with intravenous or volatile anesthetics, analgesics, and muscle relaxants (if needed). Control the gas exchange with a ventilator or squeeze the balloon by hand. Monitor vital signs: heart rate, blood pressure, SpO2, body temperature throughout the procedure.5.6 Extubation of endotracheal tube
The patient is awake and able to follow orders. Head up for more than 5 seconds and TOF >0.9 (if available). The patient is breathing on his own, the respiratory rate is within normal limits. Pulse and blood pressure are stable. Body temperature > 35 degrees C. No complications of anesthesia and interventional endoscopy.
Chỉ rút ống nội khí quản khi mạch và huyết áp của người bệnh ổn định
6. Notes when performing general anesthesia in endoscopic interventional hysteroscopy
During laparoscopy, there is a pump to the uterus, so it is necessary to monitor the amount of water entering and leaving to prevent acute pulmonary edema. Beware of perforation of the uterus or the wrong path of the laparoscope which can lead to major bleeding. Monitor for minor vaginal bleeding or spotting for a few days after the procedure, which usually resolves spontaneously. The risk of complications increases with time and complexity of the intervention. If uterine perforation is detected during the interventional hysteroscopy, laparoscopy is required to assess the nearby organs and treat according to the damage Vinmec International General Hospital is a quality medical facility. in Vietnam with a team of highly qualified medical professionals, well-trained, domestic and foreign, and experienced.A system of modern and advanced medical equipment, possessing many of the best machines in the world, helping to detect many difficult and dangerous diseases in a short time, supporting the diagnosis and treatment of doctors the most effective. The hospital space is designed according to 5-star hotel standards, giving patients comfort, friendliness and peace of mind.
Master. Dr. Ton That Quang has more than 15 years of experience working in the Anesthesia - Resuscitation industry. Doctor Quang was a doctor at the Department of Anesthesiology and Resuscitation at Khanh Hoa General Hospital and a lecturer at the provincial level of Emergency Resuscitation in Obstetrics and Gynecology before being an Anesthesiologist and Resuscitation Doctor at the Department of General Surgery, General Hospital. Vinmec Nha Trang International
To register for an examination at Vinmec International General Hospital, you can contact the nationwide Vinmec Health System Hotline, or register online HERE.