This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II To Van Thai - Emergency Medicine Doctor - Emergency Resuscitation Department - Vinmec Hai Phong International General Hospital. Thai doctor has more than 34 years of experience in the field of anesthesia - emergency resuscitation.The presence of a CSF fistula is a favorable environment for CNS infection. Therefore, intervention to close the fistula in these cases is indicated as soon as possible in the condition that the patient is under endotracheal anesthesia.
1. What is endotracheal anesthesia to close the CSF fistula?
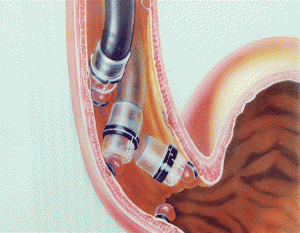
Endotracheal anesthesia is a technique of general anesthesia by performing respiratory control through intubation and the use of a ventilator. This is the method of anesthesia and sedation during surgery and post-operative resuscitation which is very common in surgery in general and CSF fistula closure in particular.Indications for the need to perform endotracheal anesthesia to close the CSF fistula are the presence of a CSF fistula or herniation of the meninges at the base of the skull by transsphenoidal or craniotomy. or by way of the ethmoid sinus. In addition, there are access through the frontal sinus or by the access route on the stony bone or postoperatively for skull base lesions.
Along with the sophisticated requirements in neurosurgery, endotracheal anesthesia to close the CSF leak requires a team of doctors with technical expertise and experience. In addition, the conditions of the surgery also need to have enough anesthetic and resuscitation facilities like general surgery. At the same time, the patient and family also need to be consulted, explained and approved for the surgery to be performed.
2. Preparation steps for endotracheal anesthesia to close the CSF fistula

Mask thanh quản là phương tiện dự phòng trường hợp đặt nội khí quản khó
Doctors, technicians and nurses specializing in anesthesiology and resuscitation.
About facilities:
100% oxygen supply Anesthesia machine system with active respiratory control function Life function monitor through ECG parameters, arterial blood pressure, SpO2, EtCO2, rhythm breathing, temperature... The means of performing emergency resuscitation such as defibrillator, sputum suction machine Surgical endotracheal intubation kit: laryngoscope, endotracheal tube of various sizes, suction tube, mask, squeeze ball, oropharyngeal canul, Magill pliers, soft mandrin. Prophylaxis for difficult intubation: Cook tube, laryngeal mask, flexible bronchoscope, tracheostomy kit, mouth opener... Local anesthetics such as Lidocaine 10% spray form . A quick-acting bronchodilator such as Salbutamol spray. About the patient:
Perform routine pre-anesthesia examination according to the procedure to detect and prevent risks related to anesthesia and surgery. Stable treatment of chronic medical conditions if any, especially Cardiovascular and respiratory management Patients and relatives are explained about anesthesia and surgical procedures; goals and possible risks around the perioperative period. Evaluate difficult intubation and plan appropriate prophylactic options. Use a sedative the night before surgery in case the patient is anxious and stressed.
3. Steps to perform endotracheal anesthesia to close the CSF fistula

Thuốc thiopental là một trong các loại thuốc thực hiện khởi mê
Check the patient
General steps:
Place the patient in the supine position and give pure oxygen at a rate of 3 to 6 liters/min at least 5 times before induction of anesthesia. minute. Installation of vital monitoring devices Establish an effective infusion with a large catheter into a fixed vein and maintain the pulse with 0.9% sodium chloride solution. Pre-anesthesia if necessary Drugs to induce anesthesia:
Sleeping pills: intravenous anesthetics (propofol, etomidate, thiopental, ketamine...) and volatile anesthetics (sevoflurane...). Analgesics: fentanyl, sufentanil, morphine... Muscle relaxants: succinylcholine, rocuronium, vecuronium... Conditions for intubation:
Patient has achieved deep sleep, sufficient muscle relaxation Intubation technique Oral trachea: Open the mouth, insert the laryngoscope to the right of the mouth, move the tongue to the left, push the light deeply, coordinate with the right hand to press the cricoid cartilage to find the epiglottis and glottis. Perform rapid induction of anesthesia and Sellick maneuver in case of full stomach (pressing the cricoid cartilage 20-30kg as soon as the patient loses consciousness until the intubation is complete). Pass the endotracheal tube gently through the glottis, stopping when the balloon of the endotracheal tube passes 2-3 cm through the vocal cords. Gently withdraw the laryngoscope. Endotracheal balloon pump. Check the correct position of the endotracheal tube with auscultation and EtCO2 results. Secure the tube with adhesive tape. Place the cannula in the mouth to avoid biting the tube.

Quy trình đặt ống nội khí quản
Choose the side of the nasal passage and apply vasoconstrictor drops (naphazoline, otrivine...). Choose an endotracheal tube size smaller than that of the oral route. Insert an endotracheal tube lubricated with lidocaine grease through the nostrils Open the mouth, insert the laryngoscope to the right side of the mouth, move the tongue to the left, push the lamp deeply, coordinate with the right hand to press the cricoid cartilage to find the rod cap. glottis and glottis. Favorable case: insert the endotracheal tube gently through the glottis, stopping when the balloon of the endotracheal tube passes through the vocal cords 2-3 cm. Use Magill pliers to guide the tip of the endotracheal tube into the correct glottis; The assistant pushes the endotracheal tube from the outside in difficult cases. Gently withdraw the laryngoscope. Endotracheal balloon pump. Check the correct position of the endotracheal tube with auscultation and EtCO2 results Fix the tube with adhesive tape. In case of difficult intubation: apply difficult intubation procedure. Anesthesia maintenance techniques:
Maintain anesthesia with intravenous or volatile anesthetics, analgesics and muscle relaxants (if necessary). Control breathing by machine or hand squeeze. CSF fistula closure technique:
Carry out dissection to reopen the surgical field following the path of the old incision Dissect the fascia and access, expose the pulp membrane Review to find the location of the torn pulp or herniated medullary membrane patching If the herniated membranous plaque is large, reconstruct it with the temporomandibular fascia Pump clean the surgical site Place drainage of residual fluid if necessary Close the incision.
4. Follow-up steps in perioperative endotracheal anesthesia to close the CSF fistula

Dựa vào nhịp tim có thể theo dõi độ sâu của gây mê
Check and be on the lookout for possible endotracheal tube misposition, flexion or obstruction.
Criteria for extubation when the patient is fully awake, has restored active respiratory function, normal hemodynamic parameters, and has no complications of anesthesia and surgery.
Monitor and manage common complications during endotracheal anesthesia such as reflux of digestive juices into the airways, trauma or respiratory inflammation... For intervention to close the CSF fistula , the patient is still at risk of recurrent cerebrospinal fluid leak or dural tear, requiring enhanced second-stage sutures.
In summary, closing the CSF fistula through endotracheal anesthesia is an indication that needs to be performed early in order to restore the structure and flow of the ventricles to the patient, and minimize the risk of CNS infection. . However, in order to achieve the highest efficiency, the surgical procedure needs to be properly adhered to as well as partially dependent on the operation of the surgeon.
Vinmec International General Hospital with a system of modern facilities, medical equipment and a team of experts and doctors with many years of experience in medical examination and treatment, patients can rest assured to visit. examination and treatment at the Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.