This is an automatically translated article.
Laparoscopic ureteral re-implantation is a treatment method for vesicoureteral reflux that is being widely applied today. This is a safe, minimally invasive procedure with few complications for the patient.
1. Overview of vesico-ureteral reflux
Primary vesicoureteral reflux is a common congenital disease. About 0.4 - 1% of children have this condition. And if counted among the causes of UTIs in children, vesicoureteral reflux accounts for 30-50%.
On the mechanism of vesicoureteral reflux: Normally, the insertion of the ureter into the bladder forms a tunnel in the bladder wall. When the volume of urine in the bladder increases, increased pressure is exerted on the bladder wall, pressing on the tunnel, preventing urine from backing up from the bladder to the ureter. When the body has congenital abnormalities, urine flow will back up from the bladder to the ureter. This long-term condition will cause urinary tract infections, irreversible damage to the kidneys, and eventually kidney failure.
The diagnosis of vesicoureteral reflux in adults and children is mainly based on cystography during urination. Based on images, people divide vesicoureteral reflux into 5 levels.
The condition of vesicoureteral reflux in children can resolve on its own during the use of antibiotics to prevent urinary tract infections if the reflux is mild. The surgical method of vesicoureteral reflux is used when urinary tract infections are recurrent, grade 4, 5, or are accompanied by other congenital abnormalities of the urinary system.
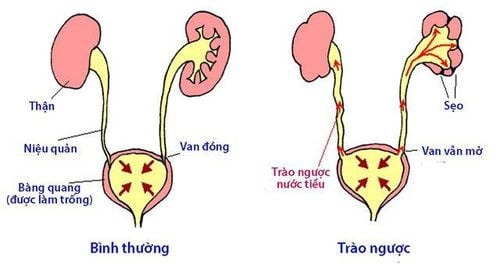
Tình trạng trào ngược bàng quang - niệu quản
2. Laparoscopic re-replacement of the ureter to treat vesicoureteral reflux
2.1 Overview of surgical methods Lich-Gregoir
There are many methods of surgery for congenital vesicoureteral reflux. In particular, the Lich-Gregoir method is the method that is being widely applied because it does not cause much damage to the bladder wall. Technically, this method creates an opening into the bladder and a submucosal tunnel for the ureter without opening the bladder.
2.2 Principles of surgery
When performing surgery, it is necessary to respect a number of principles:
Only perform surgery when the urinary tract infection is completely cured; When dissection must respect the shell of the ureter; If the ureter is dilated, it should be reshaped; The ratio of the parietal ureter to the diameter of the ureter is 4/1 or 5/1; Prophylactic antibiotic treatment after surgery for 6-8 weeks.

Phương pháp phẫu thuật Lich-Gregoir
2.3 Procedure
Surgical patients are under endotracheal anesthesia ; The patient's position is tilted to the opposite side 45°, the arms are extended along the sides of the body, the Foley urinary catheter is inserted into the urethra; Skin incision and abdominal alignment at the navel, dissection of the preperitoneal space; Insert the trocar into the opening and other trocars into the following locations: ipsilateral iliac fossa, midpoint between umbilicus and superior pubic border, contralateral iliac fossa; Find and release the ureter, bring the ureter out through the trocar hole, make the ureter smaller if the ureter is dilated; Insert the JJ catheter and fixate on the ureter; Insert the ureter and the JJ catheter into the abdomen; Inflate the bladder, split the bladder muscle at the lateral fundus until the submucosa is exposed, cut the mucosa, insert the JJ catheter into the opening of the bladder mucosa; Suture the ureter to the bladder lining; Suture the bladder muscle to tunnel and compress the underside of the ureter; Suture the peritoneum, place a drain.

Phẫu thuật nội soi cắm lại 2 niệu quản
Postoperative follow-up:
Drain drainage and discharge the patient after 2-4 days; Remove Foley urethral catheter after 7 days; Re-examination and removal of JJ catheter after 1 month; Re-examination, perform necessary tests after 2 months. Some complications:
Narrowing or obstruction of the ureter due to too narrow submucosal tunnel or angulation; vesicoureteral reflux due to too short submucosal tunnel; Necrosis of the lower end of the ureter due to damage to the blood vessels in the ureteral wall during dissection. Depending on each complication, there will be appropriate treatment interventions.

Tình trạng sức khỏe bệnh nhân ổn định sẽ được xuất viện sau 2 - 4 ngày
3. Overall rating
Laparoscopic surgery in the treatment of congenital vesicoureteral reflux according to the Lich-Gregoir method can be performed for patients with unilateral or bilateral ureteral reflux. This technique has the advantage that the bladder opening is small, so it is safe, less invasive, has a short hospital stay, and is less likely to have complications from infection, urinary leakage, and ureteral stricture. In addition, in this technique, the length of the ureter is short, avoiding complications of ischemia of the ureter.
However, in the case of thin-walled bladder and old surgical scars, the application of the Lich-Gregoir method of laparoscopic re-implantation of the ureter may be difficult.
When parents see that their child has signs of vesicoureteral reflux, they can take the child to Vinmec International General Hospital for examination and treatment. There is a team of well-trained, professional and experienced gynecologists; system of modern equipment, meeting international standards; Professional service quality, helping the diagnosis and treatment process to be highly effective.
For detailed advice on vesicoureteral reflux disease in children, please come directly to Vinmec health system or register online HERE.
MORE:
What is urinary tract infection and is it dangerous? Warning signs of UTIs Causes and signs of UTIs in children













