This is an automatically translated article.
The article is professionally consulted by Specialist Doctor II Nguyen Quoc Viet - Department of Medical Examination & Internal Medicine - Vinmec Danang International General Hospital.
Dilated cardiomyopathy is a disease of the heart muscle that is often of unknown etiology and is a major cause of heart failure. The disease has a poor prognosis with a mortality rate of 35% after 5 years and up to 70% after 10 years. So how is dilated cardiomyopathy diagnosed?
1. Diagnostic criteria for dilated cardiomyopathy
Dilated cardiomyopathy is defined when there are signs of impaired systolic function, dilated left ventricular chambers without finding common causes such as coronary artery disease, congenital heart disease, valvular disease, increased blood pressure or pericardial disease. In some cases, dilated cardiomyopathy is seen in situations such as alcoholism, pregnancy, or a family history of cardiomyopathy.2. How to diagnose dilated cardiomyopathy?
2.1. Clinical diagnosis Functional symptoms: Cough, rapid breathing are the initial manifestations of the disease. Paleness, sweating, slow weight gain, rapid fatigue and decreased urine output, and wheezing can be important symptoms of heart failure in children. Chest pain, palpitations, dyspnea on lying down, syncope, sudden death are reported symptoms (about 20% of cases), about 50% of cases of dilated cardiomyopathy have a history of previous viral infection, 25% have a family history of dilated cardiomyopathy. Physical symptoms: Children under 4 years old often have rapid breathing, light tachycardia, cold extremities, enlarged liver, low blood pressure. In some severe cases there may be shock. Children over 4 years old often have edema, bulging neck veins, rales at the bottom of the lungs, wide electrocardiogram, tachycardia, galloping sounds, and systolic murmur due to functional 2-3 leaf valve regurgitation.
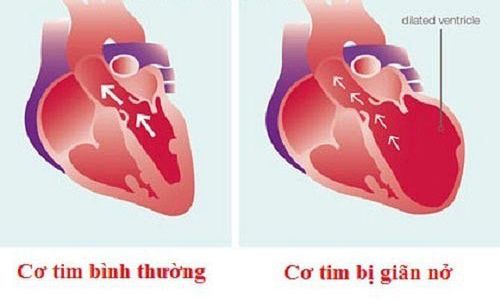
Bệnh cơ tim giãn
2.2. Subclinical diagnosis
Straight chest radiograph, enlarged heart shadow, pulmonary venous stasis, pulmonary venous hypertension, or pulmonary edema. Electrocardiogram: There are no typical ECG signs for dilated cardiomyopathy, can see irregular heartbeat such as paroxysmal supraventricular tachycardia, atrial fibrillation, atrial extrasystoles, ventricular extrasystoles. Ventricular repolarization disorder is almost constant. ST segment depression or inversion in leads D1, aVL, V5, V6, ventricular dilatation with left ventricular predominance Echocardiography: The most important method to help diagnose and monitor dilated cardiomyopathy, Besides this method can also rule out causes that can cause dilated heart chambers such as congenital heart disease, heart valve disease or coronary artery disease. 2D echocardiography of the left ventricle has a spherical shape due to more dilatation in the horizontal axis than in the longitudinal axis of the heart, the left ventricular wall thickness is reduced, all areas of the left ventricle are reduced. M Mode ultrasound showed an increase in left ventricular size at the end of systole and diastole, and a decrease in contractility and ejection fraction. Color ultrasound will show 2-3 leaf valve regurgitation due to ventricular dilatation leading to dilation of the annulus. Doppler ultrasound shows blood flow through the aortic valve, helping to estimate pulmonary artery pressure through the spectrum of tricuspid regurgitation, pulmonary valve regurgitation. Cardiovascular catheterization: Children with dilated cardiomyopathy are often at high risk of complications when angiographic catheterization. Therefore, cardiac catheterization must be performed by an experienced pediatric cardiologist. Currently the main indications for this procedure are preparation for heart transplantation and myocardial biopsy. Endocardial biopsy: Endocardial biopsy is often difficult to perform in infants and breastfed infants. In older children, endomyocardial biopsies aid in the differentiation of lesions from different etiologies. Currently, the main indications for endomyocardial biopsy are preparation for heart transplantation and monitoring of rejection response after cardiac transplantation.
Siêu âm tim tại Bệnh viện Đa khoa Quốc tế Vinmec
2.3. Differential diagnosis
In neonates, the diagnosis should be differentiated from asphyxia complicated by heart failure, aortic stenosis, aortic stenosis, systemic arteriovenous fistula, coronary artery abnormality, viral myocarditis or not due to virus.
In older children, secondary causes of cardiomyopathy should be excluded.
Dilated cardiomyopathy is difficult to detect by common symptoms, so we should get in the habit of periodically checking the health of our hearts at reputable medical facilities. Currently, in order to meet the needs of medical examination and treatment, Vinmec International General Hospital is applying the Cardiovascular Screening Package with the following advantages: Highly professional, dedicated and wholeheartedly for the benefit of the patient. With 90% holding university degrees, 20% are professors and associate professors, nearly 30% are doctorates, bringing high efficiency in medical examination and treatment. Comprehensive and professional medical examination, consultation and treatment services. A system of modern equipment, supporting effective diagnosis and treatment. Modern, civilized, luxurious and sterile medical examination and treatment space. For more details, please contact the hotlines of the hospitals or register for an online consultation with Vinmec HERE.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.