This is an automatically translated article.
The article was written by MSc Ma Van Tham - Internal Medicine Doctor, Department of Pediatrics - Neonatology - Vinmec Phu Quoc International General Hospital.Congenital airway malformation of the lung (CPAM), also known as congenital cystic pulmonary malformation (CCAM), is a rare developmental abnormality of the lower respiratory tract. Children with this malformation may present with respiratory failure in infancy or may remain asymptomatic for the rest of life. Many cases are detected early by routine prenatal ultrasound. Surgical resection is a radical treatment.
1. Clinical features
The clinical presentation of CPAM is variable. Many cases are detected by routine prenatal ultrasound. Early assessments show that up to two-thirds of infants diagnosed with CPAM antenatally have symptoms at birth.
Recent literature shows that only about 25% of children with the disease have symptoms. This disparity may reflect advances in prenatal ultrasound technology, such that small lesions can now be identified, and they are often asymptomatic.
1.1 Prenatal features The appearance of CPAM on prenatal ultrasound varies from incidental detection of cystic lesions to large pulmonary masses. Lesions that regress and appear to be reversible during pregnancy in about 50% of cases have been confirmed by fetal ultrasonography, but the majority of these are still detectable on imaging photo after birth.
Of the lesions present at birth, complete resolution of the lesions has been reported in a small number of cases. A retrospective review showed that maximal CPAM size was reached around 25 weeks of gestation and that a decrease in size was probably prognostic, unless hydrops were present.
1.1.1 Prenatal imaging CPAM is one of the most common lung lesions diagnosed before birth, despite its low incidence at birth. Prenatal diagnosis is quite specific by ultrasound. Manifestations of CPAM prenatally are classified based on ultrasound features and general anatomy.
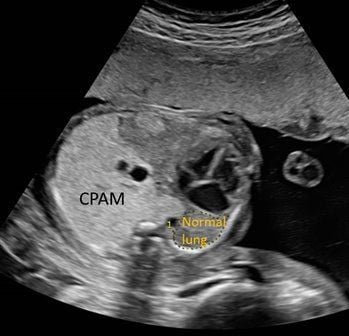
Hình ảnh chẩn đoán hình ảnh trước sinh CPAM qua siêu âm thai nhi
Small cystic lesions include forms <5 mm in size and solid ultrasound appearance, while large cystic lesions include 1 or more cysts > 5 mm in size.
CPAM volume ratio (CVR) is an indicator of CPAM volume relative to fetal head, and is a useful diagnostic indicator. Additional evaluation by prenatal MRI is valuable in differentiating CPAM from other pulmonary abnormalities, including isolated lung, congenital diaphragmatic hernia, and congenital lobar pneumothorax.
Approximately 25% of infants with antenatal CPAM detected also have other structural abnormalities, the majority of which are associated with CPAM type 2. In such anomalies, cytological karyotype should be examined. pregnant. CPAM alone is not associated with chromosomal abnormalities.
1.1.2 Fetal edema Fetal edema occurs in 5 to 40% of cases, due to hemodynamic disturbances from inferior vena cava obstruction, cardiac dislocation, and compression of surrounding structures. The risk of fetal edema is highest in fetuses with large lesions, lesions persisting into the third trimester, and lesions of small cysts. In particular, the CPAM volume ratio (CVR), which measures the volume of CPAM relative to the beginning of the pregnancy, predicts an increased risk of fetal edema.
1.2 Neonatal period 1.2.1 Asymptomatic CPAM Approximately 3⁄4 patients with a prenatal diagnosis of CPAM are asymptomatic at birth.
The natural course of asymptomatic CPAM at birth has not been well described. But it is clear that some infants are at risk of complications (mainly infections) during the first few years of life.
However, the frequency of encounters varies significantly in different cases. The risk of malignancy is very low except for type 4 lesions, although type 1 lesions have a few cases of potential malignancy. Uncertainty about the risk of infection and malignancy is the main source of inconsistency in the management of patients with postpartum CPAM.

CPAM không triệu chứng ở trẻ sau sinh trong khoảng gần một năm đầu đời
1.2.2 Symptomatic CPAM As noted, the majority of CPAM is asymptomatic, the remaining 25% of patients diagnosed prenatally as symptomatic CPAM at birth. In a series of 89 infants with a prenatal diagnosis of CPAM, 22 had signs of abnormal breathing and 12 of them presented with severe respiratory distress.
The likelihood of respiratory failure and its severity increases with the size of the lesion (eg, CVR > 0.84). Other predictors on antenatal ultrasonography of respiratory distress at birth include mediastinal compression, polyhydramnios, and ascites.
Some clinical signs associated with CPAM types are:
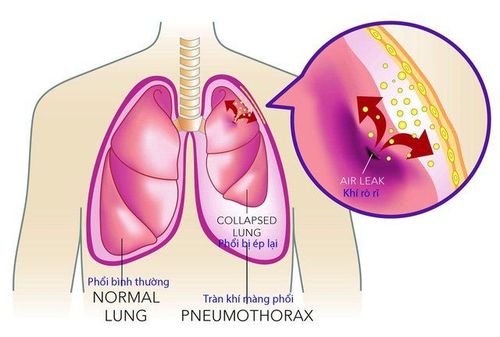
Type 0: Associated with severe impairment of gas exchange and affect neonatal mortality at birth. CPAM type 1 includes the majority of CPAM that occurs in neonates. When symptomatic, characteristic signs include tachypnea, respiratory muscle exertion with wheezing and indrawing, and cyanosis. Depending on the extent of the air trapping above, the large cyst can expand leading to respiratory failure. CPAM type 2 is often diagnosed early after birth because it is associated with other abnormalities, occurring in up to 60% of patients. Respiratory signs and symptoms appear similar to CPAM type 1. CPAM type 3 is the most severe (unlike type 0 which is fatal at birth). Type 3 lesions are large and may include the entire lung, typically with edema and pulmonary hypoplasia. The child may die at birth or shortly after birth with progressive, severe hypoventilation, cyanosis, and respiratory failure. From an epidemiological point of view, the proportion of males is much more dominant. CPAM type 4 can be present around the neonatal period and can be difficult to distinguish from type 1. Spontaneous pneumothorax has been reported in a few cases. Since many type 4 lesions are almost certainly due to pleural effusions, we must think of malignancy when an infant has pneumothorax and CPAM. 1.3 Childhood About one-third of CPAMs are diagnosed after infancy. These characteristic lesions are usually type 1, 2, and 4 and tend to be smaller than CPAMs with respiratory symptoms at birth.
A common sign in older children is repeated pneumonia. Other signs that the patient complains are cough, dyspnea, and/or cyanosis. Physical examination includes hypoventilation in the affected area, chest wall disproportion, and bulging lesion.
CPAM may present with spontaneous pneumothorax. Because pneumothorax is most commonly associated with type 4, and type 4 is associated with malignancy, we should always think about and look for malignancy in the case of patients with pneumothorax and CPAM. .
In a report of 12 patients diagnosed with CPAM aged 6 to 23 years (mean age 6.7), 9 patients presented with recurrent pneumonia, 1 case had pneumothorax and 2 cases were developed appear by chance. Among the 11 patients who underwent CPAM resection, there were 7 cases of CPAM type 1 and 4 cases of CPAM type 2.
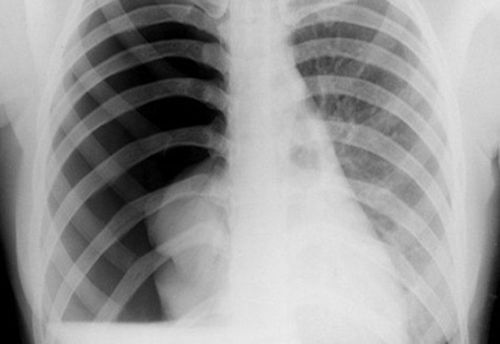
2. Diagnostic imaging

Hình ảnh CPAM trên hình ảnh cận lâm sàng
Chest CT correlates with presenting pathological symptoms. In one report, preoperative CT was compared with pathologic findings. CT accurately recognizes both small (<2cm) and large cysts, although they may be filled with air and/or fluid. The area of the solidification zone corresponds to the glandular or bronchiole structures; this was observed in 43% of cases. The area around the affected cyst is thinner and lower than the healthy lung, representing the small cysts merging with the healthy lung parenchyma; This feature is seen in 29% of cases on CT.
In summary, congenital airway malformation of the lung is a birth defect that can be detected around the 25th week of pregnancy through fetal ultrasound. Parents can screen for this malformation by having regular pregnancy health check-ups, especially in the second 3 months of pregnancy, which is the period of strong fetal development. Pregnant women need:
Comprehensive fetal malformation screening by superior 4D ultrasound technique. Screening for gestational diabetes, avoiding many dangerous complications for both mother and baby. Control the mother's weight reasonably to assess the health status of the pregnant woman and the development of the fetus. Understand the signs of threatened early delivery (especially in those carrying multiple pregnancies or having a history of miscarriage or premature birth) so that they can receive timely treatment to maintain pregnancy. To protect mother and baby during pregnancy, Vinmec provides a comprehensive Maternity service to monitor the health status of mother and baby, periodical antenatal check-ups with leading Obstetricians and Gynecologists. enough tests, important screening for pregnant women, counseling and timely intervention when detecting abnormalities in the health of mother and baby.
For detailed information about all-inclusive maternity packages, please contact the hospitals and clinics of the Vinmec health system nationwide.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.