This is an automatically translated article.
The article is professionally consulted by Master, Doctor Mai Vien Phuong - Gastroenterologist - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.III. Diagnosis by imaging and testing
1. Gastrointestinal endoscopy
The gold standard for diagnosing chronic gastritis is endoscopic imaging combined with histopathology from biopsies taken endoscopically. However, endoscopy also has some limitations such as sensitivity, low specificity and differences in image perception among doctors. However, with the use of new endoscopic techniques such as magnifying endoscopes with NBI or BLI and LCI, it is much easier to identify gastric mucosal atrophy both in extent and location. .
Normal gastric aneurysm has a subepithelial microvascular network with a characteristic honeycomb morphology. In the presence of chronic atrophic gastritis, this microvascular network is no longer visible.
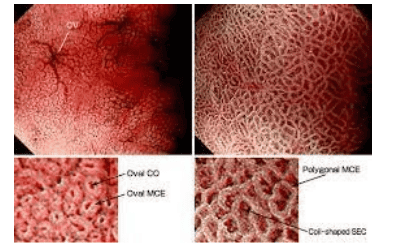
Hình ảnh niêm mạc dạ dày trên nội soi phóng đại có chức năng nhuộm màu điện tử NBI
In the early stages, it can be difficult to detect lesions on endoscopy. In the later stages, the image of pseudo-polyposis lesions can be seen on the background of atrophic gastric mucosa. If the lesion is extensive, the mucosal folds of the body may be flattened, and the submucosal vessels are more visible.
Occasionally, pseudo-polyposis lesions, hyperplastic polyps, adenoma-like lesions, and carcinoid tumors may be encountered. Carcinoid tumors appearing on the background of VDD are characterized by being small (size

Một trường hợp viêm dạ dày tự miễn được nhìn thấy qua nội soi: thân vị và phình vị mất niêm mạc, màu trắng, nhìn thấy rõ các mạch máu nằm bên dưới.
According to the recommendations of improved Sydney, take biopsies at 5 locations: 2 pieces in the body, 2 pieces in the antrum, 1 piece in the area between the body and the antrum. If the histopathology of the antrum is normal or the chronic inflammation is mild to moderate, while in the body there is a special atrophy with intestinal metaplasia, gastritis is diagnosed as autoimmune gastritis.
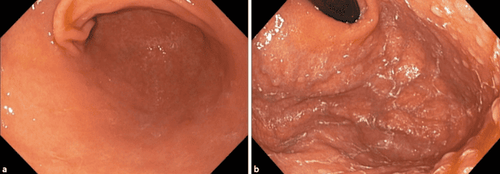
Một trường hợp viêm dạ dày tự miễn khác được nhìn thấy qua nội soi
Cases of autoimmune gastritis co-infected with HP lead to diffuse atrophic lesions of the body and antrum, in this case, the diagnosis of autoimmune gastritis is based on the results of anti-parietal cell antibodies or weak positive endogenous factor.
In addition, there are some cases with severe atrophic gastric mucosal lesions spreading to both the body and antrum while the past and present are not infected with HP.
In terms of definition, although VSD has been classified as characterized by localized lesions in the gastric body, there are still cases of patients co-infected with H. pylori leading to diffuse atrophic lesions of the whole region. flavor and taste.
In these cases, the diagnosis of VDD must be based on positive parietal cell or endogenous factor antibody results. In addition, a case series study reported that some patients had severe atrophic gastric mucosal lesions, which spread to both the trunk and antrum, while having no previous and current H. pylori infection. .
All of these patients had autoimmune or systemic diseases, so the authors suggest that the pathogenesis here is an overactive immune system that affects many types of cells. different cells in the stomach.
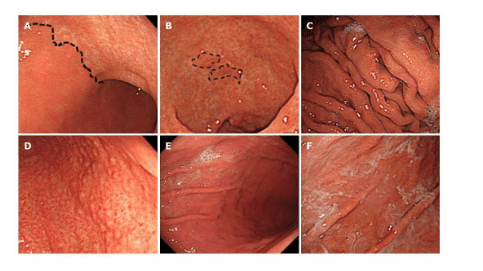
Viêm teo thân vị phía góc bờ cong nhỏ dạ dày, hậu quả của nhiễm H.pylori (Nguồn ảnh: wjgnet.com)
All of these patients have autoimmune diseases, so the authors believe that the pathogenesis here is an overactive immune system that affects many different types of cells in the stomach. .
2. Histopathology
Macroscopic assessment is mainly based on gastric specimens. In the early stages there is not much marked change in the mucosa, but as atrophic inflammation progresses, the lining of the body becomes thinner, the mucosal folds are flattened. In addition, small nodules (hyperplastic polyps, pseudopolyps, adenoma polyps, carcinoid tumors...).
Microscopically, autoimmune gastritis is a focal atrophic lesion localized to the body with intestinal metaplasia, pancreatic cystic cell metaplasia, or pheochromocytoma. In the absence of HP co-infection, the antral mucosa is normal or shows only mild reactive inflammation.
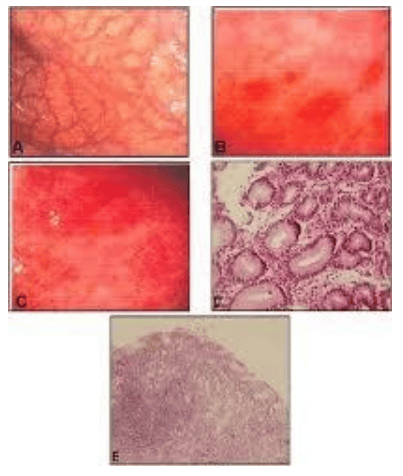
Hình ảnh mô bệnh học của viêm teo dạ dày
3. Other tests
Anti-parietal cell antibodies: Finding specific antibodies in VTE helps to screen and confirm the diagnosis more effectively. Antibodies against intrinsic factor. Quantification of gastrin levels 17 also helps to assess the state of increased gastrin secretion from G cells due to decreased secretion of gastric juice. Pepsinnogen (PG) I, II: Measuring concentration and using PGI/PGII index to coordinate diagnosis. PGI is produced by the primary cells of the gastric aneurysm, while PGII is produced by both primary and glandular cells in the entire gastric mucosa. Therefore, in autoimmune gastritis, there will be a decrease in the concentration of PGI and the index of PGI/PGII <3. Patients with macrocytic anemia should have vitamin B12, homocysteine, and methylmalonic acid measured. Serum iron.

Xét nghiệm máu giúp ích rất nhiều trong chẩn đoán viêm dạ dày tự miễn
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References
Dao Viet Hang-Dao Van Long (2018), “Autoimmune gastritis”, Autoimmune diseases – gastrointestinal allergies, Medical Publishing House. Carmel R (2996) Prevalence of undiagnosed pernicious anemia in the elderty Arch InternMed,156, 1097-200. Kulnigg-Dabsch S.(2016), “Autoimmune gastritis”, Wien Med Wochenschr 166(13-14):424-430