This is an automatically translated article.
The article was made by a doctor of Laboratory - Vinmec Central Park International General Hospital
Natural variability of the immune response; Low form factor; Determination of specificity; Transmission from mother to fetus; The effects of antibiotics... are complicated situations in serology.
1. Natural variation of the immune response
The factors influencing the immune response are many and due to factors not in bacteria and factors in the bacterium itself (beyond the details of the bacterium in itself). Given the variability of the human genome and therefore the variability in the immune system, it is not surprising that hetereogeneity in the humoral immune response to infection is not surprising. This is evident in at least the age group, the very young and the very old have less immune responses, and other reasons such as certain antigens. For example, children younger than 2 years of age may be less likely to have an immune response to bacterial polysaccharides than older children (15-17). In closed communities or in smaller genetic groups, such as families, there may be a very poor response to certain antigens or to many antigens.
Immune deficiency in some people can lead to no response, little response, or slow response. The application of serological tests must ensure that these limitations are known.

Sự biến thiên của GEN người ảnh hưởng đến đáp ứng miễn dịch
2. Rheumatoid factor
Rheumatoid factor has been described as an in vivo antibody that binds directly to other antibodies of the same host (78,79). For example, the most common form of rheumatoid factor is anti-IgM IgM. Anti-IgG IgG may also be encountered. In serodiagnostic testing, especially of the indirect type, such as the indirect EIA, rheumatoid factor may interfere with the accurate determination of whether the antibody is actually conjugated to the bacterial antigen. In the IgM test, rheumatoid factor IgM can directly combine with IgG for bacteria. When IgG is still capable of binding to the antigen (and hence the rheumatoid factor), subsequent evaluation of IgM using secondary anti-IgM antibodies may detect rheumatoid factor rather than detect IgM.
Rheumatoid factor is more frequent in human serum in patients with rheumatoid arthritis alone. In many infections, rheumatoid factor is generally generated by several mechanisms of inflammatory activity.
In at least IgM testing, rheumatoid factor can be ruled out by pre-testing IgG adsorption.
3. Determination of specificity
As described in the previous section, immunoblots are capable of serological determination of some infections. Another method to investigate the specificity of the immune response includes active serosorption of the target antigen. That is, specificity can be inferred if the antibody can be removed after reaction by precipitation with a bacterial substrate, which is usually the host bacterium. This may be easier to control with protozoan bacteria whose surface has antigenic expression rather than antigenic components (such as bacterial toxins). However, it must be standardized so that the amount of antibody to be reduced is known in advance by multiple adsorption procedures. There have been a number of examples where many suitable methods of determination have been discovered.
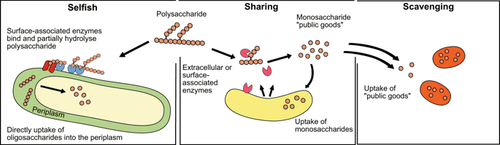
Sơ đồ nguyên lý của 3 cơ chế chính của việc sử dụng chất nền vi khuẩn
4. Maternal-fetal transfer
The mature placenta begins to let IgG cross its mother-infant barrier during the second trimester of pregnancy. Maternal IgG will be present in abundant amounts in the fetal circulation towards the end of pregnancy. IgM is a fully complex molecule that is not found in the fetal circulation unless produced by the fetus itself. Therefore, the presence of bacteria-specific IgM in the neonate or later is indicative of fetal or neonatal sepsis. Maternal IgG can persist in the infant for up to 6 months (usually about 4-12 months), and this can confound serological test results if IgG is an important target for detection. Therefore, the serological test for syphilis will often be positive in infants when their mothers are infected. Neonatal sepsis requires multiple follow-up titers at birth. Comparing mother-infant titres also has some value. Currently, there is no practical method to distinguish between maternal and paternal IgG antibodies.
5. Antibiotic effects
The immune response will typically occur during invasive disease due to most bacterial pathogens whether or not it is diagnosed. Antibiotic therapy has the potential to reduce the amount of immune response because antimicrobial resistance prevents bacterial replication and may cause the infection to end abruptly while the immune process is occurring. For many infections, which progress over time with treatment and diagnosis, multiple antibiotics will have little effect on suppressing antibody formation. There are a few examples, however, where it is believed that early treatment can slow disease progression and hinder antibiotic development. In streptococci, ASOT can be affected by the antibiotic used. Also, early administration of appropriate antibiotics may decrease serological response to Mycoplasma pneumoniae infection.

Tác động của kháng sinh làm giảm lượng đáp ứng miễn dịch
6. Humoral immune response versus cellular immune response
Using antibody measurements to indicate past infection or active infection is time-honoured. Similarly, the use of skin testing for the purpose of demonstrating a cellular immune response and therefore previous or current infection may also be applicable for a number of purposes. However, the use of in vitro cell-mediated immunological assessment has not been sufficiently explored for diagnostic purposes (80,81). It is likely that a full understanding of immunodiagnostic strategies may be biased due to the conventional methods that most studies have chosen to follow. Perhaps even the combination of 'immunodiagnostic' may be the best approach for some infections.
Invite you to follow the document on Serological Diagnosis of Infections by Doctor Tran Thi Ngoc Anh including:
Serological Diagnosis of Infections Antigens and antigenic variation Antigen relationship Voidness specificity of the humoral immune response Summary of serodiagnostic methods - Part 1 Summary of serodiagnostic methods - Part 2 General aspects of utilization in hematology Bar The Complicated Situation in Serological Diagnosis Source: Nevio Cimolai
Children's and Women's Health Center of British Columbia, Vancouver, British Columbia, Canada