This is an automatically translated article.
The article is professionally consulted by Master, Doctor Bui Tien Dat - Emergency Medicine - Cardiology - Emergency Resuscitation Department - Vinmec Hai Phong International General Hospital. The doctor has more than 12 years of experience in the field of emergency resuscitation - cardiology.Cardiac arrest or cardiac arrest is an extremely dangerous, life-threatening phenomenon. Cardiac arrest requires early intervention to prevent brain loss. There are only 3 minutes to act in the event of a cardiac arrest.
1. What is cardiac arrest?
Cardiac arrest, also known as circulatory arrest, is a sudden loss of heart function, causing the heart to suddenly stop beating due to disturbances in the heart's electrical activity. When the heart stops beating, it will lead to loss of consciousness and stop breathing, pulse cannot be caught, blood pressure cannot be measured.At this point, immediate emergency resuscitation efforts are needed because cardiac arrest will lead to death within minutes. Cardiac arrest can happen suddenly even on a perfectly healthy heart or in accidents from electric shock, drowning, anaphylaxis, multiple trauma... Illnesses can occur. both in-hospital and out-of-hospital.
2. Common causes of cardiac arrest
Ventricular fibrillation (also called ventricular fibrillation) is the most common cause of cardiac arrest complications. Ventricular fibrillation occurs when the electrical current that triggers normal heart muscle contractions is replaced by chaotic electrical activity, which results in cardiac arrest, the heart's inability to pump blood to the brain and vital organs. other of the body. Ultimately, permanent brain damage and death is possible if blood flow to the brain is not quickly restored within five minutes.Heart attack (also called myocardial infarction) is the most common cause of ventricular fibrillation.
Arrhythmia due to different causes.
Other less common but possible causes of cardiac arrest include: apnea, asphyxiation, lightning strikes, trauma, electric shock, poisoning and drowning.

Một trong những nguyên nhân gây ngừng tim điển hình là do sét đánh
3. Recognizing cardiac arrest patients
The patient is not breathing or breathing is not normal. Evaluation of circulatory arrest should not exceed 10 seconds. Patients with myocardial infarction complicated by ventricular fibrillation will lose consciousness.4. Emergency cardiac arrest at the hospital
Cardiac arrest is a serious medical emergency. Cardiac arrest mortality can be minimized through early cardiopulmonary resuscitation (CPR) and defibrillation (using electrical pulses to the chest to help restore a normal heart rhythm). In advanced countries, public places have been equipped with automatic defibrillators to perform emergency defibrillation in cases of sudden cardiac arrest.Early cardiopulmonary resuscitation and defibrillation are the only means of reversing cardiac arrest. Emergency measures must be taken within minutes of cardiac arrest.
For every minute that passes, the patient's chance of survival decreases by 7-10%. In cases of defibrillation within 5-7 minutes, the survival rate of patients with cardiac arrest has increased to 49%. Resuscitation is rarely successful if performed more than 10 minutes after cardiac arrest.
2010 AHA recommendation, use of shock energy according to the machine manufacturer's information. Many opinions suggest that the shock level should be as high as possible of the electric shock machine (usually 200J for 2-phase shockers, 360J for single-phase shock machines).
5. Emergency cardiac arrest outside the hospital

Nếu người bệnh bất tỉnh, không thở... thì cần gọi cấp cứu 115 ngay lập tức
Place the patient on his or her back on a firm surface. If the patient is lying on the stomach, turn over carefully. In case of suspected cervical spine injury, try to turn the victim over: turn the head, neck, trunk and legs at the same time. Place one hand on the center of the lower half of the victim's sternum, the other hand on top of the previous hand, alternating fingers, in the same direction. Use the force of both hands, shoulders and body to press perpendicularly to the patient's ribcage so that the sternum sinks about 4-5 cm, then lift up and continue the second beat. The optimal emergency chest compression rate is 100-120 beats/minute. Each technique of chest compressions should capture bouncing inguinal or carotid arteries (Untrained individuals should not stop to check pulse, only chest compressions and CPR), evaluate pulse does not exceed 10 seconds, should only be assessed every 2 minutes of emergency. Performing chest compressions helps push blood into the circulation by applying pressure directly on the heart combined with creating a change in pressure in the chest. In addition, chest compressions will bring blood from the right ventricle to the lungs for gas exchange, bring blood from the left ventricle to the coronary circulation and cerebral circulation, blood will passively return to the atria when compression stops, the heart relaxes and the intracranial pressure. chest is reduced.
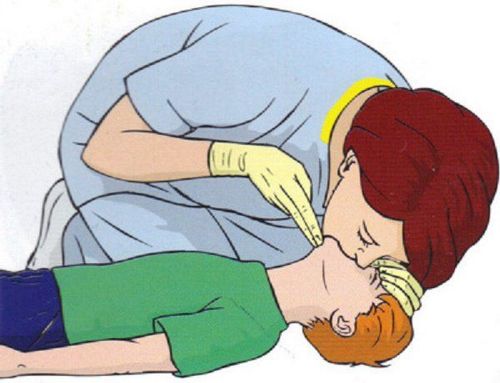
Along with the chest compressions, the person performing the first aid also needs to open the airway and give the victim asphyxiation by the technique of tilting the forehead - lifting the chin:
Put the palm of the hand on the forehead and then press it back, tilting the patient's head. Use your other hand to lift the patient's lower jaw to bring the chin forward. Mandibular thrust technique is used when the victim is suspected of having a cervical spine injury. Direct mouth-to-mouth breathing, breathing mask: use your mouth to blow air into the patient's lungs through a filter, through a mask or directly, blow slowly within 1 second so that the chest is visible. up. Initially, 2 consecutive breaths are required to assess the patient's airway patency. If the patient's thorax does not rise gently, the patient's mouth should be opened to detect the foreign body. The two movements of cardiac compression and artificial respiration must be performed alternately in a rhythmic manner, following the cycles of cardiopulmonary resuscitation.
6. Recommendations of the Vietnam Society of Cardiology
Percutaneous coronary intervention is recommended in patients with life-saving cardiac arrest and ST-segment elevation myocardial infarction ECG. nerve function. It is essential to establish a healthcare system with a professional staff to detect ST-elevation myocardial infarction patients and transfer them quickly and directly to a center capable of 24 reperfusion. /7. All healthcare professionals caring for patients with suspected myocardial infarction should have access to defibrillation equipment and training in basic cardiac arrest. Emergency coronary angiography (and interventional coronary angiography if indicated) for patients with life-saving cardiac arrest whose ECG does not have ST-segment elevation myocardial infarction but who are at high risk of developing cardiac arrest. ischemic heart disease. Rapid and large intravenous infusion of cold solutions is not recommended in patients after spontaneous circulation has been restored.Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.