This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General HospitalThe patient suffered from shortness of breath, prolonged wheezing, went to many doctors but still did not reduce the disease. It was time to see a gastroenterologist, found that the patient had reflux esophagitis, and the doctor concluded that the patient's shortness of breath and wheezing was caused by reflux esophagitis. What are the characteristics of this disease?
1. Overview of reflux esophagitis, asthma
1.1 Reflux esophagitis Gastroesophageal reflux disease (GERD) (reflux esophagitis) is a common gastrointestinal (GI) disease, with worldwide prevalence and prevalence. high prevalence in Western countries. The 2006 Montreal Consensus defined gastroesophageal reflux disease as a condition that develops when the reflux of gastric contents causes troubling symptoms and/or complications into the esophagus. Tissue damage associated with gastroesophageal reflux disease ranges from esophagitis to Barrett's esophagus and adenocarcinoma of the esophagus; The troubling symptoms of reflux can be esophageal (regurgitation, regurgitation) or extraesophageal.Gastroesophageal reflux disease can be further classified by the presence of an erosive stoma on endoscopic examination (erosive reflux disease [ERD] and non-erosive reflux disease [NERD]).
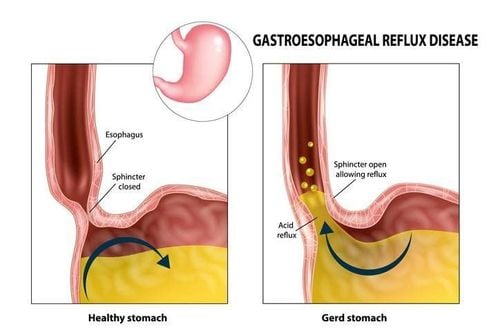
Trào ngược dạ dày thực quản (GERD) là một bệnh lý về đường tiêu hóa (GI) phổ biến
1.2 Asthma Asthma Asthma is defined by the American Thoracic Society (ATS) as “a condition with a history of intermittent episodes of wheezing, coughing, or shortness of breath and forced expiratory volume per second (FEV1). ) 20% from baseline after administration or reduction of bronchodilators, in FEV1 20% after bronchoalveolar transplantation with methacholine”.
Gastroesophageal reflux is suggested as a cause of asthma, as well as when clinically silent, and an effective GERD treatment can improve asthma control asthma.
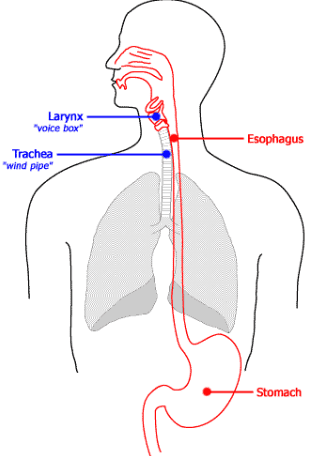
Thực quản và vùng thanh khí phế quản có liên quan trực tiếp với nhau
2. The relationship between asthma and gastroesophageal reflux disease
A significant association between asthma and GERD has been demonstrated in epidemiological studies: Up to 50% of asthma patients have associated gastroesophageal reflux disease. However, the prevalence of asthma in patients with GERD remains uncertain: Study reports range from 30% to 90%, compared with an average of 24% in controls.1 large prospective European study (GERD GERD) showed that 4.8% of patients with gastroesophageal reflux disease may have asthma, while the incidence of reflux disease Higher silent gastroesophageal reflux (24–29%) can be found in cases of difficult-to-control asthma. Broers et al. reported that the mean GERD prevalence in asthmatic patients was 46.54%, based on symptoms alone, and 52.70% based on pH and endoscopic monitoring. endoscopy, while in the control group, the rate of gastroesophageal reflux disease was 23.59% based on assessment of symptoms.
Although there is a temporal association between asthma and GERD, GERD does not always cause asthma. According to Avidan et al., half of coughs and wheezing in asthmatic patients are associated with acid reflux, and when pH is monitored for 24 hours, it is noted that reflux episodes lead to acid reflux. a cough. However, while an occasional bout of cough can rarely lead to reflux, a regurgitation that results in a cough is more common.

Có tới 50% bệnh nhân hen suyễn có bệnh trào ngược dạ dày thực quản liên quan
3. Difficulty in diagnosing asthma related to gastroesophageal reflux disease
Similarly, given the challenges encountered in chronic cough, the diagnosis of GERD-associated asthma is difficult: Upper endoscopy, pH impedance, and PPI testing when positive An association between diseases has not always been demonstrated. Silent reflux and nocturnal regurgitation are common in patients with asthma and respiratory symptoms: During sleep, the usual protective responses are absent, increasing the damage caused by reflux.An unanswered question is if asthma aggravates gastroesophageal reflux disease or gastroesophageal reflux disease worsens asthma. In asthmatic patients, many factors can contribute to the worsening of gastroesophageal reflux disease: Cough and increased respiratory effort, pulmonary hyperinflation, diaphragm contraction, and increased pressure gradient across the LES . Asthma medications such as theophylline, β-blockers, and corticosteroids can promote reflux. In contrast, gastroesophageal reflux disease as the underlying cause of asthma should be suspected in patients with adult-onset asthma, without a family history, without an allergic component, Poor response to traditional asthma medications, symptoms preceded by heartburn and regurgitation, or worsened after eating.
4. Pathogenesis of asthma related to gastroesophageal reflux disease
Asthma and chronic cough share two main theories about the association with gastroesophageal reflux disease. According to the reflux theory, the reflux of gastric juice components directly damages the lung parenchyma, causing symptoms such as coughing and wheezing, causing histological damage, which can lead to lung injury. acute lung and acute respiratory distress syndrome. According to the reflex theory, reflux stimulates the vagus nerve, leading to bronchospasm.Bronchial hyperresponsiveness is typical of asthma and is defined by abnormal bronchial constriction caused by various agents. Esophageal reflux aggravates asthma by inducing bronchial overreactivity to refluxed aspiration, esophageal-triggered vagal reflexes, and esophageal neuritis caused by lower cytokine release tachykinin form.

Trào ngược thực quản làm trầm trọng thêm bệnh hen suyễn bằng cách gây ra phản ứng quá mức của phế quản đối với việc hút chất trào ngược
5. Treatment of asthma associated with gastroesophageal reflux disease
Lifestyle changes, such as elevating the head of the bed, stopping smoking and dietary changes (reduced fat, chocolate, alcohol, citrus, tomatoes, coffee and tea, avoiding meals large and eaten 3 hours before bedtime) are recommended to improve reflux control and possibly help improve bronchial symptoms, although there are no RCTs to confirm this hypothesis.5.1 Role of PPIs in the treatment of GERD-associated asthma Although PPIs have demonstrated superiority over H2 blockers for esophagitis, they are effective of previous medications in the treatment of GERD-associated asthma remains a matter of debate: Several studies report improvements in symptoms and lung function with the treatment of reflux, while other studies have not demonstrated this effect.
In a Cochrane systematic review of randomized, placebo-controlled trials performed in patients with asthma, 6 studies investigated the effects of PPIs and 5 studies investigated the effects of the drug. H2 blocker. The authors found no clear effect on lung function, airway responsiveness, or asthma symptoms.
Although most included trials reported at least one significant outcome, there was no consistency in results: Increased FEV1, decreased use of β-antagonists significantly improved asthma symptoms, and nocturnal asthma improvement after PPIs treatment was reported by 2 or 3 studies each. Interestingly, only one trial assessed the impact of behavioral changes and one trial evaluated the outcome of surgical approaches. None of the studies reported hospitalizations or emergency room visits due to asthma. A meta-analysis, summarizing PPI treatment in asthmatic patients, concluded that there was a small but significant improvement in the rate of PEF (Peak Expiratory Flow) the morning after PPI treatment, although this improvement is likely to be of minimal clinical significance; no overall improvement in lung function and asthma symptom scores were revealed.
This meta-analysis included studies comparing asthmatics with and without a diagnosis of GERD: Both groups showed small but statistically significant improvements in PEF rates morning with PPI therapy, although greater benefit was seen in people with GERD. Differences in duration of treatment or cumulative PPI dose were not associated with better morning PEF ratio outcomes.
Controversial results regarding the effects of PPIs in asthmatic patients arise from different methods, small sample sizes, and absence of a placebo group in published studies. Currently, there is no evidence to recommend PPIs for all asthmatic patients, while patients with nocturnal asthma or nocturnal regurgitation may have some beneficial effects.
5.2 Practical treatment recommendations Practical recommendations in patients with asthma associated with gastroesophageal reflux disease (with or without esophageal symptoms) include initial empirical testing of PPIs once or twice daily for 2-3 months. In patients who respond to therapy, PPIs should be tapered to the minimum dose necessary to control symptoms. In unresponsive cases, testing reflux with pH testing or impedance-pH monitoring can rule out pathological reflux.
5.3 Role of surgery In several studies, antireflux surgery showed some beneficial effects on GERD-associated asthma: Decreased disease control scores and Asthma medication consumption decreased. However, a lack of consistent evidence encourages routine use of this method and further investigation is warranted.

Trong một số nghiên cứu, phẫu thuật chống trào ngược cho thấy một số tác dụng có lợi đối với bệnh hen suyễn liên quan đến bệnh trào ngược dạ dày thực quản
Currently, Vinmec International General Hospital has an asthma screening package for patients with bronchial asthma. Vinmec's asthma screening package helps:
Screening for early detection to promptly control and treat the disease Perform clinical examination, take medical history, measure respiratory function, otolaryngology and clinical examination bronchial filter. When registering for the Asthma screening package, customers will receive:
01 appointment with an Allergist - Clinical Immunology 01 time to perform screening tests: Measure respiratory function Measuring FeNo Endoscopy otolaryngology Allergen testing Visited by a team of Professors, Doctors, Doctors such as: Prof. Dr. Dr. Dinh Xuan Anh Tuan , Dr. Dr. Nguyen Van Dinh has a full range of professional facilities to diagnose the disease and stage it before treatment. Quick examination time, thorough consultation, easy compliance with treatment management
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
ReferencesMarilena Durazzo,1,2,* Giulia Lupi, Extra-Esophageal Presentation of Gastroesophageal Reflux Disease: 2020 Update, J Clin Med. 2020 Aug; 9(8): 2559. Vakil N., Van Zanten S.V., Kahrilas P., Dent J., Jones R., Global Consensus Group The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus. Am. J. Gastroenterol. 2006;101:1900-1920. doi: 10.1111/j.1572-0241.2006.00630.x. [PubMed] [CrossRef] [Google Scholar] Kahrilas P.J., Altman K.W., Chang A.B., Field S.K., Harding S.M., Lane A.P., Lim K., McGarvey L., Smith J., Irwin R.S., et al. Chronic cough due to gastroesophageal reflux in adults: CHEST guideline and expert panel report. Chest. 2016;150:1341–1360. doi: 10.1016/j.chest.2016.08.1458. [PMC free article] [PubMed] [CrossRef] [Google Scholar] Irwin R.S., Madison J.M. Diagnosis and treatment of chronic cough due to gastro-esophageal reflux disease and postnasal drip syndrome. Pulm. Pharmacol. Ther. 2002;15:261–266. doi: 10.1006/pupt.2002.0348. [PubMed] [CrossRef] [Google Scholar]