This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital
In order to provide accurate assessment and positive treatment direction, bringing high efficiency to patients, currently artificial intelligence techniques in optical tomography combined endoscopy and laser endoscopy have been developed. application in the diagnosis of esophageal cancer.
Abbreviation:
EC: Esophageal cancer
AI: artificial intelligence
BE: Barrett esophagus
1. Overview of the application of artificial intelligence to gastrointestinal endoscopy
Due to the rapid progression and poor prognosis of esophageal cancer (EC), early detection and diagnosis are of great value in improving the prognosis for patients. However, early endoscopic detection of esophageal cancer, especially Barrett dysplasia or esophageal squamous dysplasia, is difficult. Therefore, the demand for a more effective method to detect early esophageal cancer features has led to in-depth research in the field of artificial intelligence (AI).
Deep learning and memory techniques (DL) have brought breakthroughs in image processing, video and other aspects, while complex neural networks (CNN) have paved the way for detect high-resolution endoscopic images and videos.

Ung thư thực quản giai đoạn sớm được nhìn thấy qua nội soi

Phân chia giai đoạn của ung thư sớm thực quản
2. Application of Machine learning and Deep learning algorithms in esophageal cancer
The current demand for more effective methods of early detection and characterization of esophageal cancer has led to in-depth studies in the field of artificial intelligence (AI), which can be identified by intelligence. intelligence established by machines as opposed to the natural intelligence displayed by humans and other animals.
Machine learning (ML) and deep learning (DL) are important parts of AI. Machine learning can be divided into supervised and unsupervised methods. Unsupervised learning is to identify groups in data according to commonalities, lacking knowledge of the number of groups or their meanings. When the training package contains input/output pairs, a supervised learning model is required to map the new input to the output. Conventional ML techniques are limited in their ability to process natural data in its raw form. In the early stages of research and development, model training was mainly with ML, through which researchers had to manually extract probable disease features based on clinical knowledge. The power of this computer-aided diagnosis (CAD) system is weak and insufficient to be applied in clinical real-time diagnosis.
3. The role of artificial intelligence AI in early esophageal cancer development
3.1 Barrett's dysplasia and early stage esophageal adenocarcinoma AI AI based on white light endoscopy (WLE) and NBI narrowband endoscopy system. There are some limitations to recognizing early cancerous lesions associated with Barrett's esophagus by WLE, a common technology. High-definition WLE (HD-WLE) and the NBI endoscopy system were once considered to improve the accuracy of the diagnosis of early cancerous lesions associated with Barrett's esophagus.
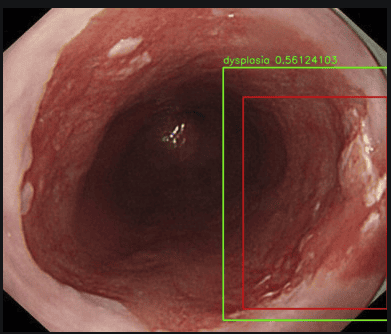
Hình ảnh loạn sản thực quản được đánh giá qua hệ thống nội soi có sử dụng trí tuệ nhân tạo AI: máy tính sẽ tìm khu trú tổn thương tự động (ô màu đỏ), đánh giá tổn thương đó có bao nhiêu phần trăm là ung thư
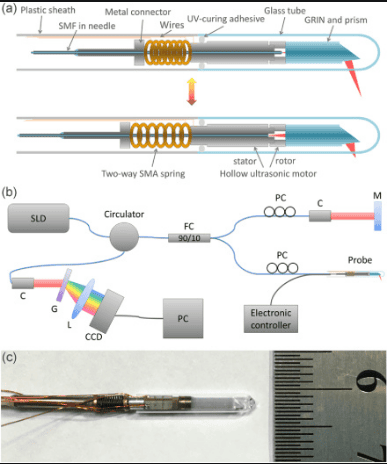
Nguyên lý và cấu tạo của hệ thống chụp cắt lớp quang học kết hợp qua nội soi (EOCT)
To solve this problem, Qi et al extracted multiple EOCT imaging features and combined one or more features to classify lesions, but the results were not satisfactory. Then, Swager et al used volumetric laser endoscopic imaging (VLE, integrated with second-generation OCT) for training and testing, and the results showed that the CAD system was superior to the one. VLE experts. Veronese et al used CLE imaging, and the results showed that the system was able to accurately differentiate gastric (GM), intestinal (IM) and neoplasia.

Mối tương quan mô học với hình ảnh chụp cắt lớp quang học kết hợp qua nội soi (EOCT)

Hình ảnh của chụp cắt lớp quang kết hợp qua nội soi (EOCT) và nội soi bằng laser đồng tiêu (CLE)
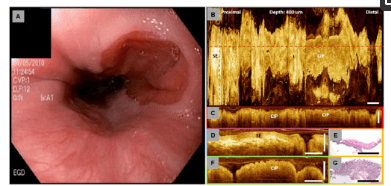
Hình ảnh chụp cắt lớp quang kết hợp qua nội soi (EOCT) của một tổn thương ở thực quản
4. AI real-time diagnosis
Currently, research in this area is limited. Ebigbo et al further optimized the CAD system based on previous research and applied it to clinical real-time detection for the first time. While 14 Barrett cancer patients underwent endoscopic examination, 62 endoscopic images (36 early esophageal carcinomas and 26 non-dysplastic Barrett's esophagus) were taken with the CAD system for real-time classification. , and the results showed sensitivity and specificity of 83.7% and 100%, respectively. There were no significant differences between the system and the experienced endoscopists.
However, there are still some shortcomings in this study. First, the number of patients and images is low. Second, the system still uses images for diagnosis, not video for real-time detection. Finally, AI's ability to aid in lesion delineation and biopsy guidance remains unproven. In addition, the CAD system built by Hashimoto et al. can meet clinical real-time detection needs. Unfortunately, the researchers did not verify the system's performance in real-time diagnostics.

Sử dụng AI trong hệ thống nội soi: Ô vuông màu xanh là máy tính tự động khu trú hình ảnh tổn thương khi đưa máy soi đến.
Tokai et al also used unmagnified endoscopic images for analysis and found that the sensitivity of NBI is slightly higher than that of WLE, and the diagnostic performance of the system is better than that of internal experts. soi. Further analysis showed that the accuracy of the CAD system in diagnosing tumors invasive to epithelial, choroidal, and muscular layers EP/LPM and MM is more than 90%, significantly higher than invasive tumor diagnosis. invades the submucosal layer SM1 and SM2. The reason may be that the training image set did not contain a normal esophageal image, and the system confused extra-frame compression and failure to fully extend the esophagus wall for lesion features.

Hình ảnh IPCL bình thường và bất thường
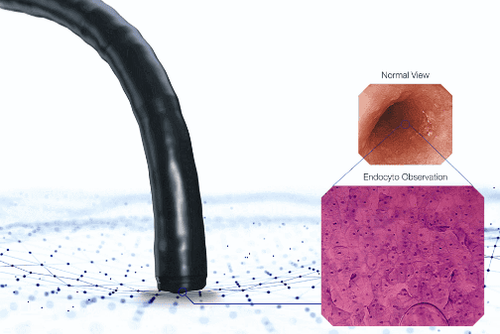
Hình ảnh nội soi tế bào
Although today's equipment and machines have been developed to help the treatment bring better results. However, the best and safest way we should maintain a healthy lifestyle, diet, and routine health check-ups to detect pathogens early so that timely intervention can be initiated.
Currently, Vinmec International General Hospital is developing screening and early detection services for gastrointestinal cancers that combine clinical and paraclinical examination to bring about the most accurate results possible.
The health check is performed by a team of experts, experienced doctors combined with NBI endoscope with anesthesia. Peripheral blood count (laser counter). Automated prothrombin time test. Activated Partial Thromboplastin Time (APTT) test using an automated machine. General abdominal ultrasound... The application of technology and modern equipment to the examination will give accurate results, make the treatment more effective, and shorten the hospital stay for the patient. core.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424. [PubMed] [DOI] Hur C, Miller M, Kong CY, Dowling EC, Nattinger KJ, Dunn M, Feuer EJ. Trends in esophageal adenocarcinoma incidence and mortality. Cancer. 2013;119:1149-1158. [PubMed] [DOI] Thrift AP. The epidemic of oesophageal carcinoma: Where are we now? Cancer Epidemiol. 2016;41:88-95. [PubMed] [DOI] Lu-Ming Huang, Wen-Juan Yang, Zhi-Yin Huang, Cheng-Wei Tang, Jing Li, Artificial intelligence technique in detection of early esophageal cancer, World J Gastroenterol. Oct 21, 2020; 26(39): 5959-5969