This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II To Van Thai - Emergency Medicine Doctor - Emergency Resuscitation Department - Vinmec Hai Phong International General Hospital.Endoscopic nerve decompression surgery for facial paralysis is a difficult technique that requires a high level of skill of the surgeon, while the operation time is quite long, although this method is not too complicated. Aim for airway control during surgery and postoperative resuscitation. Except in the case of patients with CNS lesions accompanied by poor self-awareness.
1. Indications and contraindications to perform laryngeal mask anesthesia endoscopic nerve decompression treatment for facial paralysis
1.1. Point
Laryngeal mask anesthesia is preferred in the following cases:Difficulty in using endotracheal anesthesia, especially when ventilation is difficult or impossible. Temporarily manage the patient's airway and breathing in the emergency department. Patients with VII nerve palsy are indicated for surgery to treat.
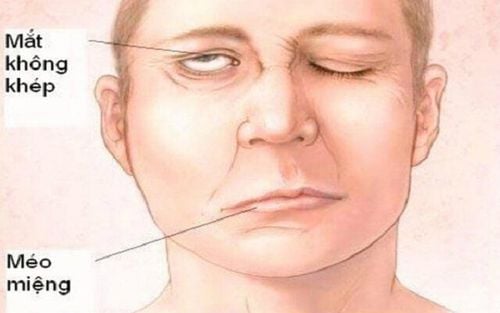
Bệnh nhân bị liệt dây thần kinh số 7 có chỉ định phẫu thuật để điều trị
1.2. Contraindications
Patients with a full stomach Face damage complicated by trauma or infection. The hospital does not have enough facilities to perform anesthesia resuscitation.2. Steps to administer laryngeal mask anesthesia endoscopic nerve decompression treatment for facial paralysis
The method is performed by a physician or nursing staff experienced in laryngeal anesthesia mask placement. The hospital must have adequate equipment for anesthesia and resuscitation. After checking the patient's profile and condition, laryngeal mask anesthesia is performed.2.1. General steps in laryngeal mask anesthesia
Put the patient in the supine position, give 100% oxygen at a dose of 3-6 l/min at least 5 minutes before induction of anesthesia. Install the tracker Set up the transmission. Pre-anesthesia (if necessary) Initiation of anesthesia: In turn inject intravenous anesthetics, volatile anesthetics, analgesics, muscle relaxants (if necessary). Conditions for placing a laryngeal mask: The patient needs to sleep deeply and have enough muscle relaxation (if necessary).2.2. Placing a laryngeal mask
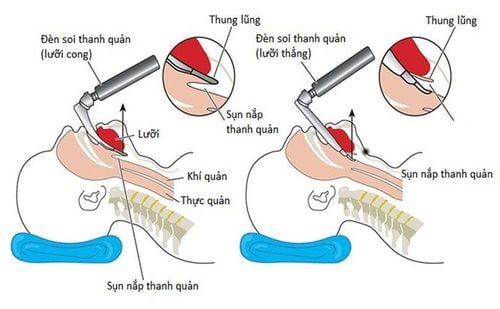
Position the patient's head slightly back. Hold the mask like holding a pen, put your index finger on the junction between the larynx mask and the tube, with the other hand open the patient's mouth. Insert the laryngeal mask through the teeth into the base of the tongue, the back of the mask against the nasopharynx. Then push the mask vertically from the palate to the hypopharynx. During the operation, if you encounter resistance, you should stop immediately. Inflate the cuff to the recommended volume. Check the tightness of the laryngeal mask after placement (can be easily ventilated and no air leak). Listen to the lungs and check the EtCO2 results to determine if the laryngeal mask is in the correct position. Secure the tube and mask with adhesive tape.2.3. Maintain anesthesia
Maintain anesthesia with initial drugs: intravenous anesthetics, volatile anesthetics, analgesics, muscle relaxants. Manual respiratory control by hand squeeze or machine. Monitor the depth of anesthesia based on parameters such as: heart rate, blood pressure, sweat, tears (PRST), MAC, BIS and Entropy (if available). Monitor vital signs of patients after anesthesia such as heart rate, body temperature, EtCO2, SpO2 values. Preventing cases of laryngeal mask occlusion, incorrect mask placement,...2.4. When can the laryngeal mask be removed?
The patient is awake and can follow the doctor's orders. Lift the patient's head for more than 5s, if muscle relaxants are used, the TOF value must be greater than 0.9. The patient is breathing on his own with a stable pulse. Body temperature above 35 degrees C No complications after anesthesia or surgery.
Thực hiện gây mê mask thanh quản
3. Some complications after laryngeal mask anesthesia and how to handle it
3.1. Stomach fluid backs up into the airways
Digestive juices can be found in the patient's oral cavity and airways. Treatment:Carry out aspiration, keeping the patient's head low and tilted to the side. Quickly insert an endotracheal tube and aspirate any fluid that appears in the airway. Monitor and prevent the occurrence of lung infections after surgery.
3.2. Hemodynamic disorders
Unstable blood pressure can increase or decrease, heart rate erratic Depending on the medical condition and the cause to take appropriate measures.3.3. Complications due to laryngeal mask placement
In the event that a laryngeal mask cannot be placed, endotracheal anesthesia should be switched.For patients with laryngeal - air - bronchial spasms:
Identify by auscultation with rales or muted lungs, difficult or impossible to ventilate. Provide adequate oxygen, increase the dose of sleeping pills and muscle relaxants, ensure ventilation. If the patient's respiratory status is critical and uncontrollable, switch to the difficult option of intubation. For some injuries caused by the laryngeal mask placement process such as bleeding, broken teeth, foreign bodies in the airways, laryngeal injuries, etc., it depends on each case to handle.

Trường hợp không thể đặt mask thanh quản chuyển sang gây mê nội khí quản
3.4. Some respiratory complications
Some complications:The laryngeal mask is slipped or folded. The respiratory system is open. The oxygen source is exhausted. Soda has no effect. Treatment: After the above respiratory complications, it is necessary to ventilate immediately and provide 100% oxygen to the patient. Identify the cause and provide an appropriate solution.
3.5. Some complications can occur after removing the laryngeal mask.
Respiratory failure Sore throat, hoarseness Constriction of larynx, trachea, bronchi. Inflammation of the upper respiratory tract The process of anesthesia mask larynx endoscopic surgery for nerve decompression treatment of facial paralysis is not too complicated. However, it requires experienced operators to identify complications and promptly handle them so as not to endanger the patient.Doctor Thai has more than 34 years of experience in the field of anesthesia - emergency resuscitation and is currently a doctor at the Emergency Department of Vinmec Hai Phong International Hospital.
Customers can directly go to Vinmec health system nationwide to visit or contact the hotline here for support.
SEE MORE
What to know about intubation in children Intubation cesarean section in patients with pre-eclampsia Intubation is indicated in what cases?