This is an automatically translated article.
The article was professionally consulted with Specialist Doctor II Dinh Van Loc - Department of General Surgery - Vinmec Danang International General Hospital.Injury to the cervical spine is a common type of injury in occupational accidents, traffic accidents, ... When an injury occurs, the most important thing and should be given top priority is to perform first aid. properly and take the patient to the nearest medical center.
1. What is anesthesia for bone graft surgery in cervical spine injury?
Bone fusion surgery in the presence of cervical spine injury is a very difficult and complicated surgery in terms of both anesthesia and surgery.The most difficult factor when performing anesthesia is the induction phase to intubate the endotracheal tube. If the movement to insert the tube is not accurate and quick, it is easy to have complications that can aggravate the injured part of the cervical spine.
Anesthesia method in Osteoarthritis surgery when cervical spine injury is general anesthesia, endotracheal intubation. To ensure a safe and technically correct endotracheal intubation process, additional aids can be used, such as a flexible bronchoscope.
Indications for general anesthesia when patients have cervical spine injuries and need surgery to fix the spine, including bone grafts.

Phẫu thuật ghép xương khi xuất hiện chấn thương cột sống cổ là một loại phẫu thuật rất khó, phức tạp
2. Anesthesia - resuscitation
Anesthesiologists may be involved in the initial airway management of patients with acute spinal cord injury, in intensive care unit resuscitation, and in the operating room for spine or surgical procedures. other art.Preoperative evaluation
Pre-anesthesia assessment should be as thorough as the urgency of the situation allows. When possible, the full extent of the patient's injury, the date of the injury, and the medical history should be considered, and airway assessment and direct physical examination should be performed.
Other injuries often occur at the time of spinal cord injury. Maxillofacial fractures, thoracic trauma, and fractures are common and may interfere with anesthetic use. For example, patients with significantly elevated intracranial pressure (ICP) due to associated traumatic brain injury may not be able to tolerate the prone position for spine fracture surgery until the cerebral edema has been treated. or in remission. Similarly, patients who develop severe acute lung injury will also require special resuscitation management. In many cases, the anesthesiologist, surgeon, and internist must discuss the relative risks and benefits associated with the duration of surgery.
Evaluation of the airway - In all the most urgent situations, an assessment of the airway should be made, including assessment of mouth opening, dentition, presence of other facial trauma, head trauma, and blood in the airways. breathing and patient cooperation. Until the cervical spine has been adequately imaged to rule out associated injuries in the trauma patient, the anesthesiologist should examine and evaluate the cervical spine for instability. When possible, imaging of the spine should be reviewed.
The patient may be immobilized with the cervical spine with a Collier brace, collar, or other device that may interfere with the ability to conceal ventilation or an airway device.
Choice of Anesthesia - In most cases, spinal injury patients will require general anesthesia for surgical procedures. For extremity procedures (eg, fusion for extremity fractures, suturing of open proximal wounds), peripheral nerve anaesthesia can be used if it can be performed without move the spine and is not contraindicated.
Monitor - Standard monitor (blood pressure monitoring [BP], capillary oxygen measurement,(SpO2) electrocardiogram [ECG], end-expiratory carbon dioxide [ETCO2], anesthetic and temperature analysis degrees) is used for all patients under general anesthesia. In addition, patients with thoracic and cervical spine injuries often require continuous BP monitoring with an arterial catheter, which should be inserted prior to induction of anesthesia to respond promptly to hemodynamic changes.
In addition to continuous BP monitoring, arterial catheterization facilitates sequential blood sampling to evaluate tests for hematocrit, coagulation parameters, electrolytes, blood gases, and blood lactate levels bar. Varying arterial inotropic impulses can provide an assessment of the patient's volume status When neurosurgery is used in spine surgery, the choice of anesthetic agent must be changed. changed to allow for optimal tracking.
Establishment of intravenous lines - It is necessary to establish intravenous lines before positioning the patient for surgery. Spinal surgery can lead to a lot of blood loss; we order two large intravenous (IV) lines (if possible, 14 or 16-gauge) to combine the instruments. We use an infusion warmer in the connection with the largest IV.
Central venous access may be indicated when necessary for adequate perfusion, and for administration of vasopressors.
Kỹ thuật đặt ống nội khí quản
3. Steps to take during Anesthesia-Skeletal Fusion Surgery in Cervical Spine Injury
The patient lies on his back, breathes 100% oxygen at a dose of 3-6l/min, at least 5 minutes before the induction of anesthesia.Initiation of anesthesia:
Sleeping pills: Intravenous anesthetics, pay attention to use etomidat or ketamine anesthetics when there is blood loss or lack of fluid. The anesthetic evaporates and maintains the anesthesia. Pain relievers such as sulfentanyl, fentanyl, ... Muscle relaxants such as rocuronium, vecuronium, Avoid suxamethonium after spinal cord injury 48g risk of hyperkalemia. Conditions for intubation: the patient sleeps deeply and has sufficient dilation muscle (in nearly all cases). *Intubation technique: nasal and oral.
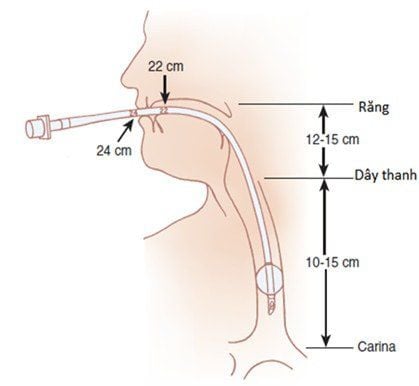
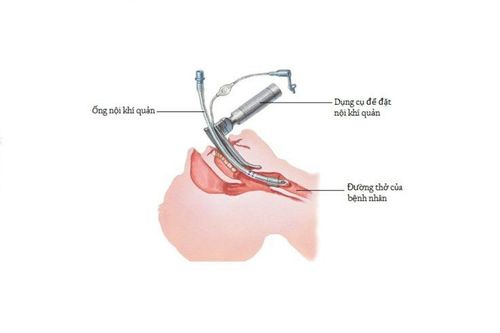
*Oral endotracheal intubation technique:
Open the patient's mouth and then insert the laryngoscope into the right part of the mouth, quickly move the tongue to the left to help push the lamp deep, at the same time pressing the right hand. cricoid cartilage to look for the glottis and epiglottis. Perform rapid induction of anesthesia and perform the Sellick maneuver in cases of full stomach (the doctor presses the cricoid cartilage for 10-30 N when the patient is unconscious until the endotracheal tube is complete). The endotracheal tube is gently threaded through the glottis and is stopped only when the balloon of the tube passes through the vocal cords for 2-3 cm. Gently withdraw the laryngoscope. Inflate the endotracheal tube slowly. Auscultation and EtCO2 results are used to check the correct position of the endotracheal tube. Secure the tube with adhesive tape. Place the canul in the mouth to prevent the patient from biting the tube. Maintain anesthesia using volatile anesthetics, intravenous anesthetics, analgesics, and muscle relaxants if necessary. Control the patient's breathing by squeezing hands or using a machine. At the same time, monitor the depth of anesthesia based on blood pressure, heart rate, tearing, sweating, MAC, BIC, ... Check vital signs such as blood pressure, heart rate, EtCO2 , ... And watch out for cases where the endotracheal tube is misplaced or folded or blocked. The standard for extubation is when the patient is awake, has a body temperature of over 35 degrees Celsius, and can breathe spontaneously within the permissible limits. And found that the patient did not appear dangerous complications of anesthesia or surgery. Complications and management
Reflux of gastric juice into the airways:
Occurrence of digestive juices located in the airways and oral cavity. Carry out aspiration, adjust the patient's head to lie low and tilt the head to one side. Then quickly intubate the endotracheal tube to clear the airways of fluid. Monitor and prevent patients from developing lung infections after surgery. Hemodynamic disturbances:
The patient has hypotension or hypertension, which may be accompanied by cardiac arrhythmias (eg, bradycardia, tachycardia, or arrhythmia). Treat the situation according to the symptoms and causes. * Complications caused by endotracheal intubation:
Can not be intubated: there is an intubation procedure that can be applied or switched to using another method of anesthesia. Misplaced in the stomach: detected when listening to the lungs, no alveolar murmurs were found and no EtCO2 was measured. Treat by reintubation. Air - laryngeal - bronchospasm: difficulty in ventilation, when listening to the lungs, there is a crackling sound or the lungs are mute. To handle it, just provide adequate oxygen for the process, add sleeping pills and muscle relaxants, ensure ventilation and add bronchodilators if necessary. However, if breathing still cannot be controlled, the CPR may use a difficult intubation procedure. * Complications of the respiratory tract:
Falling, folding, the endotracheal tube is pushed deep into a lung, causing the respiratory system to collapse or open, leading to the lack of oxygen. Treat by immediately ensuring ventilation and provide 100% oxygen immediately, detect and resolve the cause. Complications after extubation: patients have respiratory failure or sore throat hoarseness, upper respiratory tract inflammation, ... The doctor will find out the cause and treat each symptom. Surgery to combine bones and bones in cervical spine injury is a dangerous surgery, which can appear many dangerous complications, threatening the patient's life. Therefore, when there is any suspicion of cervical spine injury, the patient needs to be examined and examined, to determine the extent of the injury, thereby giving appropriate treatment.
Vinmec International General Hospital is one of the hospitals that strictly applies safe surgical anesthesia practice standards according to international guidelines. Vinmec has a team of experienced anesthesiologists and nurses, modern equipment such as: nerve detectors, ultrasound machines, Karl Storz's difficult airway control system, comprehensive anesthesia monitoring system GE's AoA (Adequate of Anesthesia) including monitoring of anesthesia, pain and muscle relaxation will provide high quality and safety, helping patients to have adequate anesthesia, not wake up, and do not have residual muscle relaxants after surgery.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.