This is an automatically translated article.
Articles written by MSc, BS. Mai Vien Phuong, Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital
Gastroesophageal reflux disease (GERD) is a major economic burden when it significantly reduces the patient's quality of life and work productivity and tends to increase in Asian countries. general and Vietnam in particular. Gastroesophageal reflux disease (GERD) in Vietnam in recent years has increased to 15.4% in patients with upper gastrointestinal symptoms, higher than the frequency of gastric ulcers (8). .2%) and duodenal ulcer (6.7%) (10). The GERD-TQ (NVDD-TQ) classification according to Hill has been shown to be a simple and useful tool for predicting gastroesophageal reflux, better than lower esophageal sphincter pressure.
Where is the esophagus located in the body? The stomach is the largest part of the digestive tract, the upper part connects to the esophagus, the lower part connects to the duodenum. Structurally, the stomach has four main parts: the cardia, the fundus, the body, and the pylorus. The cardia is the junction between the esophagus and the stomach, food from the esophagus passes through the cardia to the stomach without a closed valve, but only a mucosal fold, called the gastroesophageal valve fold. The fundus is dome-shaped, located below the diaphragm, above and to the left of the cardia. Below the fundus is the body and main part of the stomach. The funnel-shaped pylorus helps to float the stomach and duodenum. The pyloric sphincter (a type of smooth muscle) is located at the end of the junction between the stomach and the duodenum.
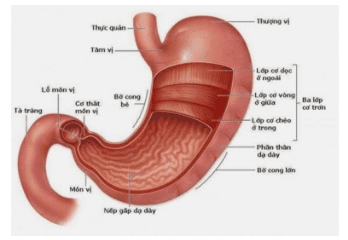
Hình 1: Giải phẫu học của dạ dày
Esophageal fissure – where is the stomach located? The gastroesophageal junction is located at the junction between the esophagus and the stomach.
During gastrointestinal endoscopy, when observing parts of the stomach in the upright position, the endoscopist will reverse the endoscope to examine the areas of the fundus, gastric cardia, then, It will be observed that the mucosal folds converge at the esophageal-stomach junction, which is the esophageal-stomach valve fold.
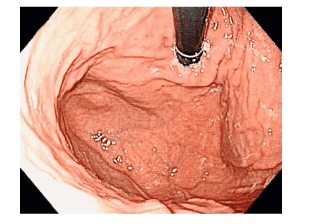
Hình 2: Hình ảnh nếp gấp van thực quản – dạ dày bình thường: lỗ tâm vị ôm chặt ống so
What is Gastroesophageal Reflux (GERD)? Esophagitis is an inflammation of the lining of the esophagus, the part of the digestive tract that connects the throat to the stomach, which is responsible for bringing food into the body. It can be caused by acid reflux, an infection, a side effect of certain medicinal products, or a food allergy that makes it difficult for the patient to swallow, pain in the chest. Gastroesophageal reflux disease (GERD) occurs when acid in the stomach regularly backs up into the tube between the mouth and stomach called the esophagus. This acidic solution can irritate the lining of your esophagus.
Association between gastroesophageal reflux disease (GERD) and gastroesophageal junction

Hình ảnh Barrett thực quản
Gastroesophageal reflux disease (GERD) is a common disorder with an incidence of about 10-20% in the Western world. The clinical manifestations of GERD (i.e., heartburn and acid reflux) are due to reflux of digestive juices in the stomach into the esophagus. The current theory of the pathogenesis of GERD is multifactorial involving the lower esophageal sphincter (LES), diaphragm, esophageal acid neutralization, gastric acid secretion, gastric emptying, and intraluminal pressure. Abdominal. The Montreal definition of gastroesophageal reflux disease (GERD) states that GERD occurs when the reflux of stomach contents into the esophagus causes symptoms and/or complications. Possible complications include esophagitis and Barrett's esophagus. In Barrett's esophagus, the normal squamous epithelium of the distal esophagus is replaced by columnar epithelium, giving rise to columnar esophageal epithelium in the esophagus. The definition of Barrett's esophagus has always been controversial and there is no universally accepted criterion. The most common definition of Barrett's esophagus requires histologically verified intestinal metaplasia at the gastro-oesophageal junction.
The gastro-oesophageal junction (GEJ) is the anatomical area where the distal esophagus joins the proximal stomach. Under normal conditions, it is in a horizontal position with the diaphragm. However, the position of the GEJ is not fixed and moves several centimeters during swallowing and breathing. During swallowing, the longitudinal smooth muscle of the esophagus shortens, resulting in a physiological hernia. The GEJ is then returned to its original position by elastic support structures, especially by the esophageal-diaphragmatic membrane. When the GEJ, along with the lower esophageal sphincter (LES) and the gastric cardia, is displaced protractedly upward into the thoracic cavity through the diaphragm, then a diaphragmatic hernia will occur. Studies have shown that hiatal hernia reduces LES pressure and diaphragmatic sphincter function. The presence and axial length of a hiatal hernia mass have also been shown to correlate with the severity of GERD.
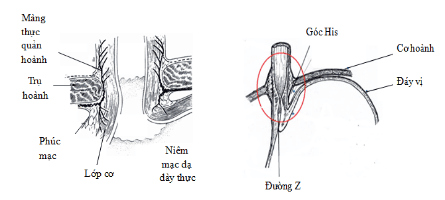
Hình 3: Cơ thắt dưới thực quản, góc His, màng thực quản – hoành đóng vai trò quan trong trong bệnh lý trào ngược dạ dày – thực quản
Hill classification for abnormality of gastroesophageal esophageal folds (NVDD-TQ) Characteristics of gastroesophageal folds (NVDD-TQ) according to Hill classification have been reported to be associated with reflux disease Gastro-oesophageal reflux (BTNDD-TQ). In Vietnam, the ratio of NTDs to TQs tends to be more and more common, but there are still very few studies on NTDs.
Characteristics of UTIs according to the Hill classification are assessed as shown in Figure 1. (A) Grade I: clear folds, the cardiac orifice hugs the bronchoscope. (B) Grade II: the folds are clear but not as good as grade I, the cardiac orifice opens and closes rapidly with respiration. (C) Grade III: The folds are not clear and the cardiac orifice does not hold the bronchoscope tightly. (D) Grade IV: no folds, the gastroesophageal junction is open, and the esophageal epithelium can be seen in the retrograde position of the nasogastric tube.
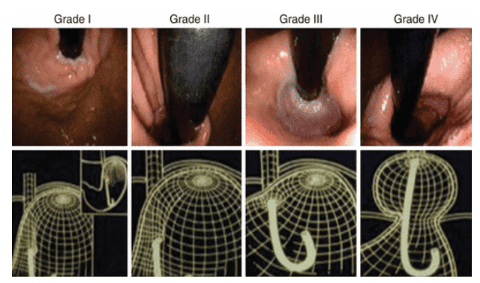
Hình 4: Phân độ của NVDD-TQ theo phân độ Hill được đánh giá như hình 1.
(A) Grade I: clear folds, cardial foramen hugging the bronchoscope. (B) Grade II: the folds are still clear but not as good as grade I, the cardiac orifice opens and closes rapidly with respiration. (C) Grade III: The folds are not clear and the cardiac orifice does not hold the bronchoscope tightly. (D) Grade IV: no folds, the gastroesophageal junction is open, and the esophageal epithelium can be seen in the retrograde position of the nasogastric tube.
Are gastro-oesophageal valve fold abnormalities common? Because the frequency of NTDs-China in Asia tends to increase. There has been a great deal of research on the risk factors for the disease in Asia. Known risk factors include: older age, male sex, smoking, obesity. Abnormal status of NVDD-TQ has also been mentioned in some studies and shows that NVDD-TQ abnormality is an independent factor related to UTI-TQ. There are few Asian data available on the frequency of NVDD-TQ abnormalities. Iwamoto et al. reported that the abnormal frequency of UTI in Japan was 13.5% with the frequency of CRC of 27% in patients undergoing upper gastrointestinal endoscopy. In another study in Taiwan, Lin et al. recorded an abnormal frequency of NTDs-TQ as 27.3% with a frequency of UTI-TQ as 41.3% in healthy subjects undergoing screening gastroscopy. . According to a study by a few authors in Vietnam, the abnormal frequency of valve folds is: 36.2% with most of them being grade III, very few cases in grade IV. Similar to previous studies in other populations, the authors also noted abnormal NVDD-TQ as an independent risk factor for UTI-TQ. This result contributes to explain why the frequency of UTI-TQ tends to be higher in the populations with a higher frequency of TNDD-TQ. A recent study comparing two groups of Caucasian Russian and Korean patients also found that NVDD-TQ abnormalities were also an independent risk factor for UTI regardless of race. According to many studies , anomalies of the valve folds are more common in men than in women, more common at the age of <40 years than in the age of 40. according to age while some other studies have not found a relationship between age and abnormality of valve folds. This relationship still does not have a satisfactory explanation, so it still needs to be studied further in the future.
Is there a relationship between abnormal gastroesophageal fold and obesity? Many studies of the authors have not recorded an association between abnormality of valve folds and obesity, abdominal obesity, smoking or drinking alcohol.
Role of esophagogastroduodenoscopy in evaluating abnormality of the gastroesophageal valve folds. Esophagogastroduodenoscopy (EGD) is the standard evaluation method for examining the upper gastrointestinal tract. The ability of the mechanical anti-reflux barrier can be evaluated endoscopically in two ways; One way is to measure the axial length of any hiatus hernias present (between the hernia cleft and the gastroesophageal junction). Because of the physiological kinetics in this region, it can be difficult to measure the length of the diaphragmatic hernia, even under ideal conditions. It is unclear when the length at which a diaphragmatic hernia will become clinically significant, i.e. pathologically significant, and because the GEJ is not fixed, most endoscopes use 2 cm as the diagnostic threshold. between normal and abnormal. Another way to evaluate GEJ is to classify the gastroesophageal valve fold (GEFV) using the Hill classification. Studies have shown an association between the Hill score and the frequency of GERD. A high Hill grade is also associated with low lower esophageal sphincter pressure, an increased frequency of hiatal hernias, and is likely to predict poor response to treatment with proton pump inhibitors. The Hill classification has been shown to be relevant, useful, and informative when evaluating patients with suspected GERD. Esophagitis can be identified endoscopically and classified according to the Los Angeles (LA) classification.
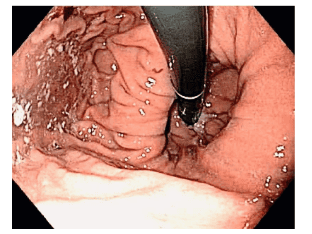
Hình 5: Một trường hợp bệnh nhân có viêm thực quản trào ngược không đáp ứng điều trị với thuốc kháng tiết axit, có nếp van thực quản – dạ dày được phân độ Hill 4.
In addition to known risk factors for reflux esophagitis such as being overweight or obese, smoking, drinking alcohol, eating fried and spicy foods, eating right before going to sleep... Gastroesophageal reflux has also been reported as an independent risk factor for this pathology. At the same time, valve fold abnormalities also help predict the patient's response to treatment.
Vinmec International General Hospital is a prestigious address trusted by many patients in performing diagnostic techniques and treating diseases of the esophagus - stomach, colon and rectum... Along with that, at At Vinmec Hospital, the diagnosis through colonoscopy with the Olympus CV 190 endoscope, with NBI function (Narrow Banding Imaging - endoscopy with narrow light frequency band) results in pathological analysis images. mucosa more clearly than conventional endoscopy, detecting abnormal mucosal lesions at an early stage. Vinmec Hospital with modern facilities and equipment and a team of experienced experts who are always dedicated in medical examination and treatment, customers can be assured of gastrointestinal endoscopy service at General Hospital. Vinmec International Faculty.
Customers who are interested in gastrointestinal diagnostic services at Vinmec and need advice and support, please book an online examination at the website or contact Vinmec's hotline for detailed advice.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.