This is an automatically translated article.
The article is professionally consulted by Dr. Nguyen Dinh Hung - Diagnostic Imaging - Department of Diagnostic Imaging - Vinmec Hai Phong International General Hospital.When detecting a bone tumor, patients often worry whether it is a benign or malignant bone tumor. X-ray imaging techniques will assess the damage when the patient has it.
1. General characteristics
Most bone tumors are benign. However, there are some tumors that can turn into malignancies, such as stage 3 giant cell tumor. The most common age of bone tumors is young and middle age, some types of bone tumors have Genetic factors. Surgical removal of the tumor when:
● The tumor is abnormally large, painful (easy to cancerous)
● The tumor is large, compressing nerves and blood vessels and limiting the range of motion of the joints.
Aesthetic influence.
2. Benign bone tumors
Chondrosarcoma Endochondritis
Giant cell tumor

Hình ảnh u nội sụn ở bàn tay trên phim Xquang
Chondroblastoma
3. Diagnosis of bone tumors
3.1. Chondrosarcoma ● Location: osteochondrosis accounts for at least 45% of benign bone tumors. Tumors tend to occur in the medulla oblongata, but can also occur in the spine and ribs, most commonly in the medulla oblongata. Tumors are common on the lower end of the femur and the upper end of the humerus is usually slow growing.
● Age: patients are usually under 20 years of age at the time of first detection.
● Characteristics: many congenital osteochondrosis tumors are related to genetic factors. This tumor tends to bend long bones and is usually slow growing. Tumor regression occurs in 5 - 15% of cases in this group, but there are also many cases of growth
X-ray image of bone: pedunculated mycelium, starting at the medulla near the growth cartilage , and is often tilted away from the joint. This lesion in adulthood rarely extends posteriorly. Therefore, if the tumor suddenly grows in size, it is necessary to have a biopsy and have a treatment plan.
● Surgical treatment of tumors causing local discomfort or compression, including removal of the tumor stalk. Secondary tumors require complete removal, and in rare cases amputation may be necessary.
3.2. Endochondritis ● Location: Endochondritis is mainly found in the hand, including the metatarsal and finger bones, followed by the upper arm bone.
● Age: the rate is similar in men and women, and accounts for about 10% of all benign tumors. Endochondral tumors are most common in the age group of 10 - 70 years, with an average age of about 30 years.
● Characteristics: slow natural progression and less likely to cause pathological fractures. Tumors in places such as the collarbone, small bones in the hands and feet, and tumors in other places are difficult to feel or see.
● Bone X-ray image: cystic, lesion extending down the bony body in long bones. There was no periosteal reaction. The presence of calcified spots in the cyst is characteristic. Macroscopically they are hard gray-white granules, transparent.
Treatment with curettage and bone graft

Một tổn thương ở đầu dưới xương đùi có vôi hóa lốm đốm không đều điển hình của chất nền sụn
3.3. Giant cell tumor ● Location: Giant cell tumor (TBKL) is a common tumor around the knee, sacrum, lower radial head and upper arm bone.
● Age: male/female ratio is 3/2.
● Features: spontaneous progression, no treatment, will lead to giant tumor, pathological fracture, and possibly skin necrosis above the tumor. Virtually not seen until cartilage closure develops. Tumors tend to be centrally located in the growing cartilage and extend around. The main symptom is pain, rarely seen in pathological fractures.
● X-ray image of bone: can be seen in the form of cysts expanding around. The trabecular bone is normal, the area of bone destruction is shaped like a soap bubble, with little periosteal reaction. The lesion is filled with orange-brown soft tissue, without calcification. This tumor can recur and become malignant.
Surgical treatment to remove the tumor. The disease can be completely cured. Surgical curettage and bone grafting are the current standard treatment methods. The risk of recurrence is 40%. If recurrence, biopsy is needed to re-define the tumor type. Surgery should be performed when the tumor is at risk of malignancy to remove the tumor. Surgical curettage to remove the tumor and graft with bio-cement is not effective. Radiation therapy also has little effect due to the risk after radiation therapy.
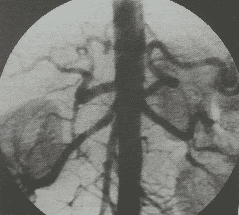
3.4. Hemangioma in bone ● Location: hemangioma in bone is common in the metaphysis of long bones and in the spine, especially in the posterior arch.
● Age: usually around 20 years old. The male/female ratio is equal.
● X-ray image of bone: shows an eccentric lesion containing an enlarged cyst with many niches. Small cavities with thin walls inside. Tumors are seen as blood holes with thin membranes at the border.
● Characteristics: The main symptom is pain and swelling. Pathological fractures are uncommon. These tumors usually destroy locally, but do not metastasize.
● Treatment includes surgery to remove the tumor. Radiation therapy is applied only to lesions that are difficult to be operated on. The probability of recurrence is about 30-60%, and depends on: the surgery to remove the tumor, the age of the patient (usually the risk is higher in patients under 15 years old), and the size of the tumor (the larger the tumor, the risk of recurrence). the higher).
3.5. Solitary bone cyst ● Location: solitary bone cyst can occur at any age. This is a benign lesion that is likely to heal on its own.
● Age: mostly seen in children from 5 to 15 years old. Male/female is 3/2.
● X-ray image of bone: showing bone cysts with many compartments, especially radiolucent, at the top of bone or near growing cartilage. The crust is usually thin, with no periosteal reaction. Often pathological fractures have little or no displacement
● Characteristics: bone cysts are mainly fluid with thin crust, the fluid can be serum or blood. Lesions also vary, from large to small, sometimes detected on radiographs while looking for other pathologies. This lesion usually extends along the diameter of the medulla oblongata. Spontaneous pathological fractures occur in 15% of cases. Tumors are usually asymptomatic until a pathological fracture occurs.
● Treatment: in the past, treatment was usually curettage of tumor and autologous bone graft. Recurrence is common in 20 to 50% of cases, and the rate is twice as high in children under 10 years of age as in children over 10 years of age. Active cysts have a higher risk of recurrence after surgery and a greater risk of developing cartilage plate damage. The technique of methylprednisolone injection is a new and safe technique after surgery. The results are positive with a recurrence rate of 5-10%, and few complications.
Expected results until pathological fracture heals, and biopsy is needed. Although biopsy is difficult because the lesion is really small, it should be differentiated from a solitary tumor.

Một tổn thương tiêu xương rõ, vị trí trung tâm ở đầu gần xương đùi. Đây là hình đặc trưng cho nang xương đơn độc
3.6. Chondroblastoma ● Location: Cartilage growth around the knee and upper arm bone is a common site. Pain that radiates into the joint is the primary symptom, with possible local swelling and associated limitation of joint motion.
● Age: 90% of cases are from 5 to 25 years old. Male/female is 2/1.
● X-ray image of bone: showing bone destruction. This lesion does not grow and enlarge like giant cell tumors. Often non-invasive tumors cross the growth plate despite closing the growth plate with age. This lesion develops eccentrically in the metaphysis, and has calcified contours within the tumor.
● Treatment is by surgical curettage and bone grafting. The recurrence rate ranges from 10 to 40%. If recurrence, continue to remove tumor and bone graft. There is no evidence that radiotherapy and chemotherapy are effective for chondroblastoma
● Features: Benign bone tumors are mostly treated with surgery. When there is a tumor, the patient should be examined for early detection and timely treatment before the tumor really affects the motor function of the patient.
Patients with bone tumors can go to Vinmec International General Hospital for examination and treatment. There is a team of musculoskeletal specialists who are well-trained, experienced and professional; system of modern equipment, meeting international standards; Professional service quality, high efficiency in diagnosis and treatment.
For benign bone tumors: It is very important to examine, diagnose and detect lesions since there are no clinical signs or new clinical manifestations. Benign bone tumors can affect the quality of life of patients if not detected and treated in time: Persistent pain, morphological changes of bone structure, spontaneous fractures... Therefore, early examination, early and accurate diagnosis is essential.
At Vinmec hospital system with modern equipment, a team of doctors and nurses with good qualifications and international standard medical examination and treatment process. Patients will be scheduled for examination and screening as well as developing a detailed treatment and recovery plan. With the spirit: CUSTOMER CENTER. Patients will enjoy professional service quality, high efficiency in diagnosis and treatment.
Doctor Nguyen Dinh Hung has over 10 years of experience in the field of diagnostic imaging (Ultrasound, CT, MRI). Trained and practiced on hepatobiliary interventional radiology at Bach Mai Hospital (Intervention under ultrasound guidance, DSA, CT...) and deployed at the Diagnostic Imaging Department of Viet Tiep Hospital Hai Phong. Currently, he is a doctor at the Diagnostic Imaging Department of Vinmec Hai Phong International General Hospital.
If there is a need for consultation and examination at the Hospitals of the National Health System, please book an appointment on the website to be served.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References: phauthuatxuongkhop.com