This is an automatically translated article.
The kidneys are bean-shaped organs located on either side of the abdomen. The kidneys are responsible for producing hormones and filtering water and waste out of the body. In some conditions, a nephrectomy is performed to remove all or one of the kidneys.1. In which case is the total nephrectomy performed?
Total nephrectomy is highly technical and is performed by urologists and surgeons. This technique is indicated in the following cases:Patients with ectopic kidneys. In patients with horseshoe-shaped kidney, the kidney part has complications of loss of function. Patients with giant hydronephrosis, hypoplastic or aplastic kidneys. Patients with polycystic kidney dysfunction or complications. Patients with hypertension due to renal vessels: Narrowing, atrophy of the renal arteries, renal atrophy. Endoscopic resection of a living donor for kidney transplantation. In addition, total nephrectomy is also contraindicated in the following cases:
Patients with grade IV hydronephrosis and contralateral kidney disease. Patients with pyelonephritis due to acquired or congenital urinary tract disease. The patient had a history of severe medical disease and was unable to receive anesthesia and anaesthesia. Patients with a history of previous interventions in the retroperitoneal space on the same side (through open surgery or laparoscopic surgery) such as: removal of kidney stones, shaping the pyelonephritis - ureter...
2. How is total nephrectomy performed?
Total nephrectomy includes two techniques: laparoscopic surgery and conventional surgery. Depending on the patient's condition, the doctor will choose the most effective method of implementation.Laparoscopic surgery often has advantages over conventional surgery such as:
Less pain than conventional surgery. Faster recovery time.
3. Laparoscopic surgery to remove the whole kidney
3.1. Preparation Laparoscopic total nephrectomy is performed by urologists, surgeons and technical means as follows:Karl-Storz Laparoscopic System: 0o Straight Type Laparoscope and 30o tilt, Tricam camera, unipolar and bipolar electrocautery. Ultrasonic knife. Instruments include: Trocar 5mm and 10mm, reducer 5mm, clip with tab, no tab, laparoscopic forceps, clip clamp, retractor, auto-cutter stapler, 5mm and 10mm titanium clips, hemolock. Before proceeding with the technique, the patient should be fully examined in basic tests and assessed for compensating renal function through the following tests:
Computed tomography, ultrasound, static urogram Urinary system vasculature to determine pathological etiology and evaluate bilateral renal function. Determine the cause by retrograde ureterostomy. Determine the percentage decrease or loss of kidney function by radioisotope. Identifying hypertension due to atrophy and narrowing of the renal arteries by renal artery Doppler ultrasound, renal angiography The doctor needs to improve the patient's condition before surgery in case the patient is old, weak, and exhausted. 3.2. Procedure: Patient's position: The patient is placed on the side 750 in the case of transperitoneal laparoscopic surgery and on the 900 side in the case of retroperitoneal laparoscopic surgery, the opposite lumbar rib is padded.
Anesthesia: The doctor administers anesthesia to endotracheal intubation and inserts a urethral catheter before performing surgery.
Perform the technique:
The doctor places the trocar as follows:
Transperitoneal surgery: In the case of right kidney surgery, the doctor uses 4 trocars and 3 trocars in the case of left kidney surgery. The doctor performed a small peritoneal opening, placed the first 10mm trocar next to the umbilicus, this is the camera position with a 30o lens, two 10mm trocars are placed above the iliac crest and below the costal margin, 1 5mm trocar is placed in the middle of the line. navel and sternum. Retroperitoneal surgery: The doctor placed a 10mm trocar by the open method in the position above the iliac crest above the mid-axillary line to use a camera with a 30o lens, a 10mm trocar was placed at the lower end of the XII rib and one The 5mm trocar is placed above the anterior axillary line so that the 3 trocars merge into a triangle. After placing the trocar, the doctor proceeded to create the retroperitoneal space as follows: Incision of the skin 1cm at the trocar site, the doctor used Pince to separate the muscle fascia into the SPM space, insert the self-made balloon with a gloved finger and inject 400-600 ml. air to expand. The doctor uses a wide surgical instrument to place the next trocar.
The doctor conducts nephrectomy through the following methods:
Peritoneal endoscopy. Retroperitoneal endoscopy. In case of nephrectomy for transplantation: The doctor conducts a pair of renal peduncles with EndoGIA, Hemolock. The kidney after resection is taken out through a small opening in the abdominal wall connecting trocar 1 and trocar 2, or after laparoscopic surgery, the doctor will open the abdominal wall first, clamp the renal peduncle with a posterior vascular Clamp. then cut open and remove the whole kidney.

Phẫu thuật cắt toàn bộ thận chỉ định đối với người bệnh có thận lạc chỗ
4. Surgical technique usually removes the whole kidney
Laparoscopic total nephrectomy is performed by urologists, surgeons, and technical facilities including major surgery and vascular kits.Before performing the technique, the doctor needs to clean the surgical area and explain to the patient the purpose and possible complications when performing the technique.
Common nephrectomy surgery is done through the following steps:
4.1. Anesthesia The doctor administers spinal anesthesia or general anesthesia to the patient.
4.2. Patient position The patient is placed in a 90-degree position with a pillow at the waist.
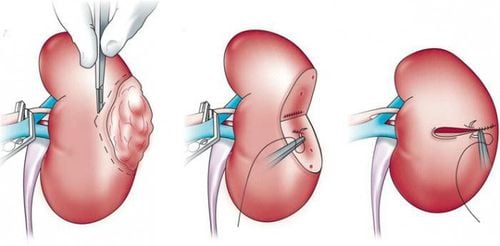
4.3. Carrying out the technique Surgical incision:
The doctor makes an incision in the lumbar spine on the side to remove the kidney and ureter with a length of 20 cm. The wide incision makes it convenient to remove the entire renal cavity mass and internal organs such as kidneys, adrenal glands, fat and the first segments of the lymphatic vessels. The doctor chooses the appropriate incision from which to determine the location and distance to remove lymph nodes and lymph nodes. After separating the renal peduncle, renal artery and renal vein respectively, the doctor performed a ligation of the renal peduncle. This maneuver is difficult to perform because the blood vessels are often surrounded by fat, have many lateral circulations or crowded with veins. Exposing the renal stem and peduncle:
The doctor conducts separate tying of the artery and vein, ensuring safety and mandatory for the complete dissection of the renal peduncle, freeing the blood vessels to have the necessary distance. The doctor performed the first arterial ligation before the vein to avoid blood stasis in the kidney. After successful nephrectomy, the doctor needs to remove the fatty tissues around the kidney and the pathological organizations in the lumbar region that are the cause of infectious complications. The drainer should preferably order a copy with multiple drains.

Cắt toàn bộ thận được thực hiện bởi bác sĩ chuyên khoa tiết niệu
5. Monitoring and managing complications of total nephrectomy
5.1. Patient monitoring Surgeons need to monitor the patient during surgery through the following factors:Pulse, arterial blood pressure and central venous pressure of the patient. Blood O2 and CO2 levels. The amount of blood to be transfused and the amount of blood lost in ml through aspiration and swabbing. After successful surgery, the patient should be monitored postoperatively as follows:
The doctor needs to monitor the patient's general condition such as hemodynamics, postoperative pain, abdominal condition, quantity urine, re-establish gastrointestinal circulation, quantity of fluid through drainage. Thrombophlebitis of extremities: Patient has fever, red edematous extremities. In this case, the doctor should perform a Doppler ultrasound of the internal iliac vein or the veins of the lower extremities. Doctors need to monitor the condition of the patient's incision for infection with the following conditions: The patient has a fever, the incision is swollen and red. Monitoring of pulmonary infarction: The patient suddenly had difficulty breathing, rapid pulse, low blood pressure, chest X-ray showed blurry results in the lungs. 5.2. Complications and management Some complications can be encountered after total nephrectomy and the treatment is as follows:
Bleeding in the abdomen (intra-abdominal, retroperitoneal): In this case, the doctor needs to perform surgery. right back. Thrombophlebitis: The doctor uses anticoagulants and antibiotics for the patient, instructs the patient to raise the leg. Doctors manage pulmonary infarction by intensive resuscitation, mechanical ventilation, use of anticoagulants and antibiotics for the patient. In case of fluid accumulation or residual abscess in the abdomen (intraperitoneal, retroperitoneal): The doctor conducts ultrasound to determine the exact location and size of the collection, for the fluid collection, the abscess has a large size. If the size is less than 5cm, the doctor can aspirate under ultrasound guidance. For fluid collection, large and deep abscess, the doctor conducts drainage or surgically cleans the abscess. Laparoscopic nephrectomy is a difficult technique that requires modern machinery. Therefore, Vinmec International General Hospital is now equipped with a new generation Dexflex Robot system with a flexible robot arm that allows surgeons to perform many precise and flexible operations when cutting and suturing wounds. , clamps, welds, CO2 suction pumps... Robots can perform complex surgical techniques that other endoscopic surgery methods are difficult or impossible to perform.
Also here, the doctors who directly perform laparoscopic nephrectomy of the Department of Surgery, Vinmec Hospital are leading experts in urology, such as: Specialist II Nguyen Minh Quang, Master Doctor Nguyen Tan Cuong... helps to diagnose and treat the disease accurately, minimizing complications after surgery.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.