This is an automatically translated article.
Artificial heart valve replacement surgery includes traditional thoracotomy, minimally invasive laparoscopic valve replacement, and valve replacement by vascular intervention. Care after artificial heart valve replacement surgery should pay attention to the treatment drugs as well as careful monitoring to avoid complications.
1. Notes when choosing artificial heart valve replacement
Patient's age Currently, for bioprosthetic heart valves, the recommended age limit is over 60 years old because at this age, the rate of degeneration of biological heart valves is much slower than in people under 60 years old. Meanwhile, patients under 60 years of age with no contraindications to anticoagulation should be considered for mechanical valve replacement.
Pre-existing disease The patient's attitude towards anticoagulant use is important in valve selection. Physicians should clearly explain the benefits and risks of anticoagulation before prosthetic heart valve replacement surgery is performed. If the patient has a contraindication or cannot control the use of the drug such as a psychiatric patient, in a remote area, the patient refuses to cooperate, etc., a biological valve should be selected.
In contrast, diseases that are at risk of thrombosis, including left atrial enlargement, atrial fibrillation, intracardiac thrombus, history of thrombosis, etc., are already indicated for long-term anticoagulation. These patients should choose a mechanical heart valve because after prosthetic heart valve replacement, anticoagulation will also be prescribed for life.
Pregnancy Using anticoagulants after prosthetic heart valve replacement has a risk of fetal malformations in the first 3 months of pregnancy. During the first 6 weeks of pregnancy, warfarin is probably safe, but the risk of fetal malformations may appear between 6 and 12 weeks of pregnancy. Therefore, prior to prosthetic heart valve replacement surgery, the benefits and risks should be carefully weighed in choosing a heart valve for young women and those planning to become pregnant. Biological heart valves avoid the risk of fetal malformations, but the disadvantage is that the heart valve will degenerate quickly and have to be re-operated to replace a new valve in an earlier time than a mechanical heart valve. If the mother is pregnant late, when the biological heart valve has degenerated, it can make heart failure worse.
If a mechanical heart valve is selected, the patient can avoid the risk of valve degeneration but must stop taking anticoagulants during the first 3 months and after 36 weeks. Instead, parenteral anticoagulants such as Heparin will be used and close monitoring is required. This is very difficult to apply to patients who are far away, do not have good medical care and monitoring conditions.
Type of surgery Choosing the type of surgery to replace the prosthetic heart valve is an important decision that affects the post-operative care for the patient.
Open thoracic surgery: This is a traditional and popular surgical method around the world, used to replace or create a heart valve using an artificial heart-lung machine. The thoracotomy method has the advantage of being easy to perform, easy to deal with, and applicable to all types of valvular heart disease. Due to the need to cut the sternum, the main limitations of this type of surgery are large surgical scars, the risk of sternum inflammation, slower recovery, and poor aesthetics.
Laparoscopic valve replacement: This is a minimally invasive surgical method. Therefore, laparoscopic surgery has the advantages of small surgical scars, high aesthetics, no risk of sternum inflammation and quick recovery. However, the technique of laparoscopic valve replacement is more difficult, takes more time, costs more and is only used for some valvular diseases but not all.
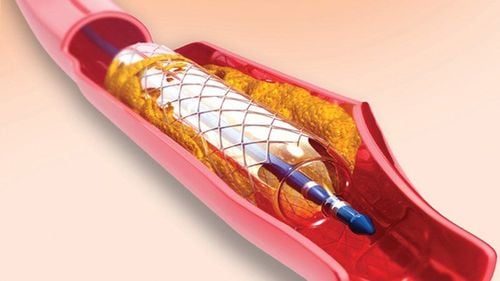
Replace heart valve with vascular intervention: this is a small surgery, so there is no need for an artificial heart-lung machine, minimally invasive and fastest recovery. The disadvantage of this method is its high cost, indicated for certain valvular diseases and the need for specialized machinery.
Dùng thuốc kháng đông sau thay van tim nhân tạo có nguy cơ gây dị tật thai nhi ở 3 tháng đầu của thai kỳ.
2. Notes after replacing the artificial heart valve
Risk of thrombosis Patients with prosthetic heart valves are at high risk of thromboembolic complications such as peripheral vascular thrombosis or cerebral embolism causing cerebral infarction. Thromboembolic complications causing valvular obstruction were also encountered in 0.3-1.3% of cases. These complications have serious consequences for prosthetic heart valve carriers.
The risk of thrombus formation in patients with mechanical heart valves is often higher than with biological heart valves, patients with mitral valve replacement are higher than aortic valve replacement, valve replacement less than 3 months has a higher risk The patient has had a valve replacement for a long time. The risk of thrombosis is also increased in the presence of other comorbidities such as atrial fibrillation, left heart failure, left atrial dilatation, history of embolism, and presence of hypercoagulability.
Anticoagulants After prosthetic heart valve replacement does not mean that the patient will be completely cured without any drug treatment. Patients with prosthetic heart valves should be treated and maintained with anticoagulation for a duration depending on the type of valve being replaced.
Today's biggest advantage of mechanical heart valves is high durability. However, wearers of mechanical prosthetic heart valves are at increased risk of thromboembolism. Therefore, patients are required to adhere to long-term anticoagulant therapy. In contrast, prosthetic heart valves are biological valves with a low risk of thrombosis, so they do not require long-term anticoagulation but have the limitation of poorer durability due to valve degeneration.
Commonly used anticoagulants are sintrom or warfarin, dose adjusted based on INR quantification. For patients with prosthetic heart valves, the INR is maintained between 2 and 3. If lower than 2, there is a risk of blood clots. An INR greater than 3 increases the risk of bleeding. Ideally, during the first 3 months after prosthetic valve replacement surgery, the INR should be maintained between 2.5 and 3.5 with any mechanical valve. After 3 months, INR should be maintained 2 to 3 for low-risk and intermediate-risk mechanical aortic valves. If a mechanical mitral valve or a mechanical aortic valve is high risk, the INR should be maintained between 2.5 and 3.5. In some very high-risk cases, anticoagulants can be combined with aspirin. In the case of patients with biological valves, during the first 3 months after prosthetic valve replacement, the INR should be maintained between 2 and 3 for the aortic valve and between 2.5 and 3.5 for the mitral valve. . After 3 months, patients with a bioprosthetic valve may no longer need anticoagulation if there are no other associated thrombotic risks.
Increased risk of bleeding during noncardiac surgery In patients taking anticoagulants, the risk of bleeding is increased with noncardiac surgery. Procedures such as tooth extraction that can ease bleeding may not require complete discontinuation of anticoagulation. However, there are some surgeries that require discontinuation of anticoagulation. The optimal time to stop the drug depends on the INR level. For major bleeding surgeries, warfarin is usually stopped 48 to 72 hours so that the INR falls below 1.5 and restarted 24 hours after surgery. If the patient is at very high risk for thrombosis such as a mechanical mitral valve, warfarin should be stopped 72 hours before surgery and heparin should be started immediately when the INR falls below 2.0 and then stopped 4 to 6 hours before surgery. surgery and restart anticoagulation as soon as hemostasis has stabilized and maintain until the INR reaches target.

Sau thay van tim nhân tạo bệnh nhân cần duy trì sử dụng thuốc kháng đông với thời gian tuỳ thuộc loại van được thay.
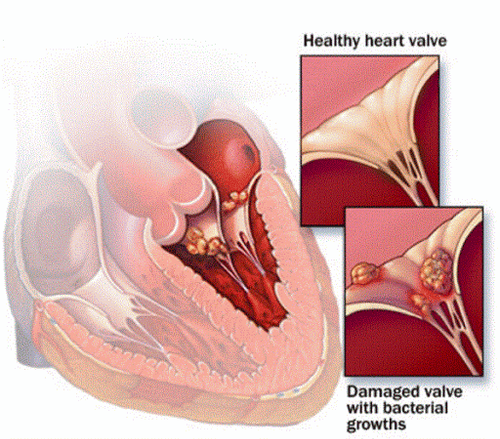
Prophylaxis of infective endocarditis Patients with prosthetic heart valves are at high risk for infective endocarditis. Therefore, prophylactic antibiotic therapy is required when performing oral, endoscopic, and other surgical procedures. Patients should also be educated about the importance of oral hygiene.
For patients with a history of infective endocarditis, the use of a biological or allogeneic heart valve is recommended to reduce the risk of recurrent infection in the postoperative period.
Postoperative follow-up echocardiography After prosthetic heart valve replacement, echocardiography should be performed immediately after discharge, 30 days after surgery, every 6 months. Echocardiography monitors patients with prosthetic heart valves whenever the patient presents with unusual symptoms such as fatigue or shortness of breath.
Other tests In addition to the INR quantification, the most commonly performed tests are the measurement of BNP levels to evaluate heart failure and the exercise test to assess exercise capacity as well as early detection of heart failure in pregnant patients. artificial heart valve.
Diet and exercise Care after surgery to replace an artificial heart valve should pay attention to nutrition and physical exercise. The diet is similar to that of patients with other cardiovascular diseases such as reducing salt, reducing saturated fat, eating more vegetables, fiber and whole grains, but limiting the intake of dark green vegetables because of the risk of heart disease. may reduce the effect of anticoagulants. Patients after surgery to replace an artificial heart valve need to have a recovery time of several weeks. Strength training in the early stages should be gentle, avoid exerting too much, do not carry heavy objects. Exercise intensity can be gradually increased according to endurance as the body recovers. In addition, the patient's psychology also needs to be comfortable and optimistic, which will help the recovery process go faster.
Vinmec International General Hospital is the only place in Vietnam that is equipped with a Hybrid room equipped with advanced equipment such as DSA angiography machine, anesthesia machine with integrated hemodynamic monitoring software. (PiCCO system, entropy,...). Therefore, Hybrid operating room can meet the requirements of surgery and angioplasty, coronary stenting, aortic stent graft, open heart surgery, heart valve replacement for congenital heart diseases with the least invasive technique. , safe to help patients recover soon.
Vinmec's cardiology team works in unity and mutual support, doctors Nguyen Van Phong and doctors Le Duc Hiep who participated in the surgery were all trained directly by foreign experts.
Vinmec is also the only place in Vietnam awarded the certificate of "Independent aortic valve replacement center in Vietnam" and GS. Vo Thanh Nhan is the first interventional cardiologist to be awarded the "Proctor" certificate in Vietnam. Vinmec's further goal is to become an excellent interventional cardiology center according to US standards, integrating with the world's level of cardiovascular intervention.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
Reference source: suckhoedoisong.vn