This is an automatically translated article.
The article was professionally consulted by Specialist Doctor I Tran Cong Trinh - Radiologist - Radiology Department - Vinmec Central Park International General Hospital. The doctor has many years of experience in the field of diagnostic imaging.Intestinal malrotation are abnormalities caused by incomplete rotation and fixation of the intestine, which occur during fetal development. Intestinal malrotation is a relatively uncommon malformation of the gastrointestinal tract. Clinically, it usually manifests in neonates and young children, but may remain asymptomatic until volvulus occurs.
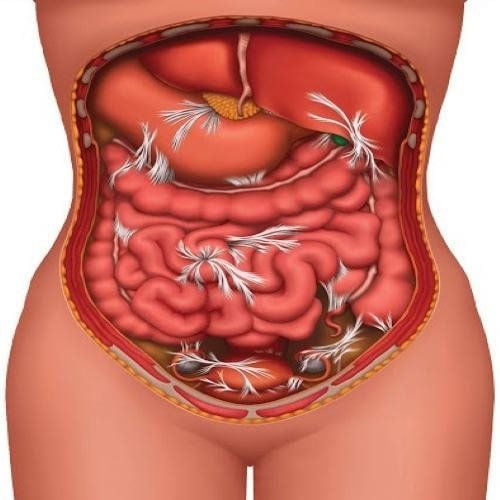
1. Anatomy and Embryology
During the embryonic stage, the intestines are located outside the abdominal cavity and in the amniotic cavity. About 10-12 weeks, the intestine re-entered the abdomen, rotated counterclockwise 270 degrees around the axis of the mesenteric vessels. At this time, the bowel loops will move to the correct anatomical position. The cecum will move towards the right iliac fossa and the duodenum lies to the left of the spine. Then the process of fixing the duodenum and colon.2. Diseases
About 60% of bowel malrotation presents with intestinal volvulus. Approximately 30% occurs in the first week of life, 60% in infants under 1 month, and 75% in infants under 1 year of age.The most common is intestinal incomplete rotation at 180 degrees, the cecum is located in front of the duodenum, at this time the mesenteric root will be shortened, leading to torsion of the entire small intestine. The anterior duodenal ligament (Ladd's ligament) will compress causing duodenal obstruction not from the inside but from the outside.
More rarely, if the bowel is not rotated, the common mesentery is present and the entire small intestine is on the right and the entire colonic framework is on the left. Usually discovered incidentally and usually without complications.
3. Clinical manifestations
There may be no clinical manifestations. Acute symptoms with high intestinal obstruction, vomiting green liquid (due to intestinal volvulus or Ladd ligament insertion), irritability, abdominal distension, dehydration, abdominal pain. Chronic presentation with chronic abdominal pain, chronic pancreatitis, weight loss, growth retardation, anorexia, intermittent diarrhea or hematuria.
Biểu hiện mãn tính với đau bụng mạn tính, viêm tụy mạn, sụt cân, chậm tăng trưởng,...
4. Methods for diagnosing rotator cuff abnormalities
4.1. Question: Acute Bile Vomiting in a previously perfectly healthy neonate. Nonspecific symptoms may be: chronic abdominal pain, chronic pancreatitis, weight loss, growth retardation, anorexia, intermittent diarrhea or hematuria. May be asymptomatic and clinically asymptomatic. 4.2. Physical examination If the bowel is incompletely rotated without volvulus, there are usually no physical symptoms.Intestinal malrotation with volvulus with the following symptoms:
Abdominal distention (distention of the stomach and duodenum secondary to duodenal obstruction). Children are often irritable, which may show dehydration (due to vomiting and loss of fluid into the third body cavity). Circulatory volume loss, small bowel ischemia progresses, the child quickly enters septic shock, at this time can see manifestations such as: erythema in the abdominal wall, peritonitis, hypotension, respiratory failure, hematemesis, melena or both, systemic metabolic acidosis, thrombocytopenia, leukopenia. 4.3. Ultrasound Normally, the superior mesenteric vein is located to the right of the superior mesenteric artery. In a patient with intestinal malrotation, the superior mesenteric vein lies to the left of the superior mesenteric artery. However, a small percentage of the superior mesenteric vein remains to the right of the superior mesenteric artery.
When there is a complication of volvulus, the image of torsion of the superior mesenteric vein around the superior mesenteric artery (whirlpool sign). To view the mesenteric vessels, color Doppler can be used for identification.
There are also other signs such as dilatation of the duodenum, dilatation of small bowel loops, decreased peristalsis, thickened bowel wall, fluid between intestinal loops, .....
4.4. Unprepared X-ray In the case of acute volvulus, a double shadow (gastric and duodenal balloon) is present, with little air in the lower bowel loops. This nonspecific image can be seen in duodenal atresia or obstruction due to a non-perforated septum.
In chronic volvulus or duodenal obstruction due to the ligament of Ladd, there is a double shadow and air in the lower bowel loops.
4.5. X-ray of gastro-duodenal esophagus Contraindicated in case of acute intestinal volvulus. Also indicated in cases where the diagnosis is doubtful:
Intestinal malrotation with a picture of the duodenojejunal angle located anteriorly or to the right of the spine. Image of torsion of the first part of the jejunum in the case of chronic torsion. The entire small intestine is located on the right side, which, in the case of the common mesentery, is uncomplicated. Abnormal gastrojejunostomy position of bowel with incomplete rotation:
Straight film: The duodenojejunostomy angle does not cross the left midline of the left vertebral column (vertebra at the level of the duodenum). The duodenojejunal angle is located lower than the duodenal bulb. Tilt film: The segments D2 and D3 of the duodenum are not posterior (retroperitoneal position).

Bụng chướng là triệu chứng của bệnh ruột xoay bất toàn có xoắn ruột
4.7. Computed tomography showed an abnormality of the superior mesenteric artery (smaller and more circular)/associated with the superior mesenteric vein. The large intestine is on the left and the small intestine is on the right.
5. Treatment
Timing of surgery: Symptomatic non-volatile malrotation should be operated on as soon as possible because of the risk of torsion.Intestinal malrotation without volvulus and no symptoms, elective surgery can be arranged after stabilization of other disorders.
Intestinal malrotation with torsion requires immediate emergency surgery.
Principle of surgery: Remove the torsion in the opposite direction of the torsion. Intestinal anastomosis when bowel necrosis. Cut Ladd's ligament. Extend the mesenteric leg. Prophylactic appendectomy. Bring the entire small intestine into the right side, the cecum and colon on the left side of the abdomen. Laparoscopic surgery is possible in cases of incomplete rotator cuff failure.

Ruột xoay bất toàn không xoắn có triệu chứng thì phẫu thuật càng sớm càng tốt vì có nguy cơ xoắn
Results of the patient's examination will be returned to the home. After receiving the results of the general health examination, if you detect diseases that require intensive examination and treatment, you can use services from other specialties at the Hospital with quality treatment and services. outstanding customer service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.