This is an automatically translated article.
The article is written by Master, Doctor Mai Vien Phuong - Gastroenterologist - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.
Computed tomography colonoscopy - virtual colonoscopy (CT Scan C) has become an important screening method in the detection of colon polyps and colorectal carcinoma (CRC). The main advantages of virtual colonoscopy are its non-invasive nature and high pathological assessment.
1. The introduction of virtual colonoscopy
Computed tomography of the colon, also known as virtual colonoscopy (VC), was introduced in 1994 by Vining et al. They were the first to describe this modified computed tomography (CT Scan) test of the large intestine as a diagnostic test for colorectal cancer and polyps. Since then, virtual colonoscopy has become a test of essential importance in the imaging of polyps and occult colorectal cancer in patients unadapted to optical colonoscopy.
Virtual colonoscopy has advantages over colonoscopy because of its less invasive nature, better patient compliance and high ability to detect extracorporeal disease. Therefore, virtual colonoscopy is an accepted screening test for colorectal cancer and is increasingly used.
We must note that, none of the findings on virtual colonoscopy allow us to distinguish adenomas from noncancerous polypoid lesions, such as hyperplastic or inflammatory polyps, so histological studies Learning is necessary in all cases.
One of the limitations of virtual colonoscopy is that it often misses flat lesions such as flattened polyps. The image is misinterpreted and can mimic polyps, including unlabelled stools, partially distended clumps, or dense folds. On the other hand, colonoscopy is often associated with anxiety, fear, and discomfort compared with virtual colonoscopy and carries a risk of incompleteness, especially in older patients. Despite these advantages of virtual colonoscopy, ionizing radiation is the most significant burden of this technique. However, improvements in imaging technology, favorable cost analysis, and the impact of peripheral results make this technique a suitable alternative to colonoscopy for cancer screening. Colorectal .
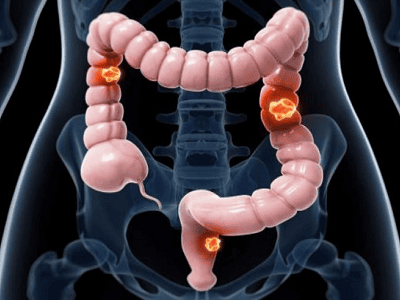
Nội soi đại tràng ảo giúp sàng lọc ung thư đại trực tràng.
2. Virtual colonoscopy after colonoscopy does not fully survey the colon
One of the generally accepted indications for virtual colonoscopy is to complete a colonoscopy after an incomplete colonoscopy (not fully surveying the colon). Approximately 10% of cases of laparoscopy cannot be completed due to various causes, eg stricture due to primary tumor, diverticular disease, adhesions, torsion loop.
One study revealed that 4.3% of tumors were missed due to incomplete colonoscopy and were found in additional imaging studies. Furthermore, proximal colon studies are particularly important in tumor stenosis, due to the high incidence of synchronous cancers (4%-5%). In some patients, colonoscopy can be technically challenging, with the inability to reach the cecum, resulting in an incomplete image of the entire colon, thereby posing a risk. Potential colon cancer and undetected polyps.
With the exception of radiology practice with an active screening program, an incomplete colonoscopy examination probably accounts for the majority of virtual colonoscopy requests. Factors that have previously been shown to contribute to the risk of incomplete colonoscopy include:
Elderly patients. Low body mass index. Female gender. History of previous abdominal and pelvic surgery. Have severe diverticular disease. Poor bowel preparation. Endoscopy experience. Tumor occlusion of the entire lumen and complications related to anesthesia. There are two main strategies regarding the timing of virtual colonoscopy after incomplete colonoscopy. They are:
The first and most common type is a virtual same-day colonoscopy using a previous colonoscopy preparation, often supplemented with oral contrast after recovery from a colonoscopy. This is often a more convenient option for the patient as they do not have to do extra preparation. Virtual colonoscopy is usually done after 2–3 hours. Another option is to have the patient return for a virtual colonoscopy at a later date using the standard protocol of virtual colonoscopy with dual contrast. Virtual colonoscopy should be delayed if endoscopic resection of the lesion has been performed during colonoscopy.

Hình ảnh nội soi đại tràng ảo
3. Screening for colorectal cancer
Most population-based colorectal cancer screening programs target ages 50 - 74 and include indirect screening, such as fecal occult blood testing or direct imaging with endoscopy. flexible sigmoidoscopy. The most common are stool-based testing [fecal occult blood test (FOBt) or fecal immunochemical test (FIT)] because of its low cost, availability, safety, and ease of transport (over-the-counter). post office).
If positive, FOBt and FIT are often followed up with colonoscopy to confirm neoplasia or suspected polyps. As virtual colonoscopy has become an available alternative to colonoscopy, many patients choose virtual colonoscopy as a more desirable option.
In a multicenter survey of 1417 individuals, 68% chose virtual colonoscopy over colonoscopy due to its less invasive nature; 47% chose virtual colonoscopy to avoid the risks associated with colonoscopy.
Another Dutch study found that 93% of patients would choose another virtual colonoscopy after the initial virtual colonoscopy. The colorectal cancer screening potential of virtual colonoscopy has been studied in three randomized European trials, including: The CCEOS study in the Netherlands (virtual colonoscopy versus colonoscopy) ), SAVE, and the PROTEUS study in Italy.
The SAVE study compared virtual colonoscopy, FIT, and fully prepared colonoscopy, while the PROTEUS study compared virtual colonoscopy and sigmoidoscopy. Participation rates, positivity rates, and virtual colonoscopy detection rates were similar across studies. Participation rates for virtual colonoscopy screening were higher than those for colonoscopy, with slightly lower detection rates, but comparable yields per invitee. The participation rate for virtual colonoscopy screening is much lower than that of FIT, but its detection rate is three times higher than that of the FIT test.
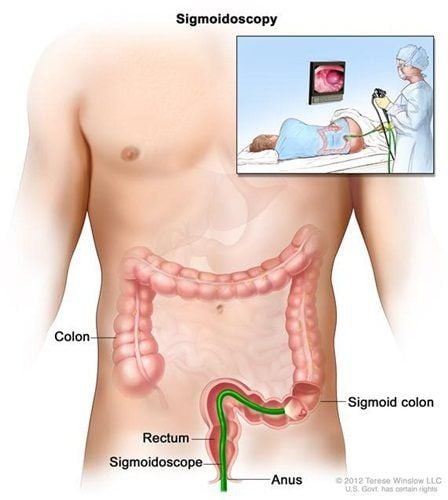
Nội soi đại tràng sigma sàng lọc ung thư đại trực tràng
4. Risk of radiation exposure
The main disadvantage of virtual colonoscopy is ionizing radiation. Radiation dose significantly determines CT Scan image quality, diagnostic accuracy, and clinical utility. Radiation dose reduction strategies are used to maintain and improve image quality. The dose should be reduced only if the diagnostic image quality can be preserved for the specific disease. Therefore, the relationship between image quality and radiation dose for radiation dose optimization in virtual colonoscopy needs to be scrutinized.5. Conclusion
Virtual colonoscopy is safe, less invasive and has a cancer detection rate comparable to colonoscopy. When performed with minimal radiation dose, virtual colonoscopy will not pose a cancer risk to the patient.
"Good practice" virtual colonoscopy includes personalizing the scanning technique according to the extent of the patient's impairment; Use the appropriate tube potential selected by advanced automatic exposure control techniques that regulate the current of the tube.
Implementing iterative reconstruction in daily clinical practice can yield improved image quality and reduced radiation dose compared with conventional filtered posterior projection-based reconstruction algorithms. State-of-the-art CT Scan equipment allows authors to perform virtual colonoscopy with much lower doses, from 1 to 5 mSv. These doses are comparable to 1-2 chest radiographs and are well above the annual radiation background in some countries. As screening programs mainly consist of two readers (two experienced radiologists) and "double-blind" readings, new perspectives arising from the integration of artificial intelligence in CT Scan machines can used for virtual colonoscopy screening instead of a "second reader".
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References:
Popic J, Tipuric S, Balen I, Mrzljak A. Color computed tomography and radiation risks: How much can we reduce? World J Gastrointest Endosc 2021; 13 (3): 72-81 [PMID: 33763187 DOI: 10.4253 / wjge.v13.i3.72]
Vining DJ , Gelfand DW. Non-invasive colonoscopy using spiral CT Scan, 3D reconstruction and virtual reality. Presented at the 1994 meeting of the Association of Gastrointestinal Radiologists, Maui, Hawaii; February 13-18, 1994.
Pickhardt PJ, Yee J, Johnson CD. Computed tomography CT Scan: more than two decades from discovery to practice. Abdom Radiol (NY). 2018; 43 : 517-522. [ PubMed ] [ DOI ]
Obaro AE , Plumb AA, Fanshawe TR, Torres US, Baldwin-Cleland R, Taylor SA, Halligan S, Burling DN. Prevalence of colorectal cancer after imaging or time interval cancer after CT colonoscopy: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol . 2018; 3: 326-336. [ PubMed ] [ DOI ]
Pagés Llinás M , Darnell Martín A, Ayuso Colella JR. [CT Scan: what radiologists need to know]. X-ray . 2011; 53 : 315-325. [ PubMed ] [ DOI ]