This is an automatically translated article.
Article written by MSc Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
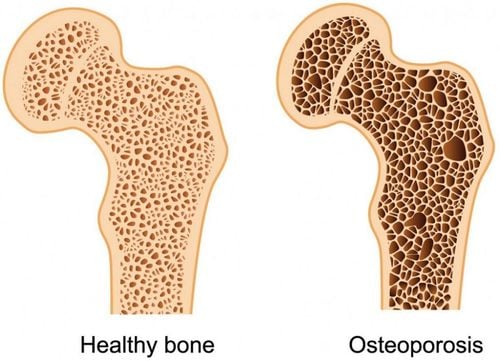
Eosinophilic esophagitis (VTQDBCAT) is an eosinophilic infiltration of the esophagus that causes clinical symptoms. Treatment of eosinophilic esophagitis is complex and requires a combination of factors.
1. Treatment goals
Treatment goals for VTQDBCAT include:
Reducing and eliminating symptoms. Improve quality of life. Prevent complications. Prevention of recurrence. Understanding the disease progression of each case is important. For patients with new progression, lesions are still localized, short-term treatment and post-treatment follow-up are appropriate, while patients at the time of diagnosis have become chronic or have complications, intervention Early and maintenance treatment should be instituted.
During treatment, monitoring response based on which criteria is still controversial. To date in most studies, response to treatment has been primarily based on improvement in clinical symptoms and reduction in BCAT counts.
However, improving the patient's symptoms in the presence of choking or dysphagia is not easy to assess because the patient can change his/her diet or there are patients whose symptoms worsen in episodes. Therefore, it is also necessary to combine with the changes in endoscopic and histopathological images.
According to the 2013 American Gastroenterological Society recommendations, histopathological complete response was defined as when the BCAT count was less than or equal to 6 cells/field or >90% reduction in the BCAT count.
Most studies use the maximum number of BCAT counts, some use the mean. In addition, it is necessary to pay attention to other characteristics related to inflammatory tissue damage such as basal proliferation, subepithelial fibrosis...
The development of endoscopic and tissue severity grading scales Pathology is expected to provide effective tools for monitoring response after treatment.

Điều trị viêm thực quản bạch cầu ái toan cần đảm bảo những mục tiêu nhất định
2. Selection of initial treatment modality
Currently as recommended by the European Society of Gastroenterology in 2017, the initial treatment modalities of choice include proton pump inhibitors, topical steroids, and diet. If there is no improvement in both clinical symptoms and histopathology, it is possible to change to a good treatment. In patients with esophageal stricture or annulus, consideration should be given to esophagectomy.
Each method has its own advantages and disadvantages for the doctor to consider and discuss with the patient before deciding on treatment. The average time to evaluate the effects of the drug/diet is 6-12 weeks.
3. Therapeutic drugs
3.1.Proton pump inhibitors (PPIs) From 2006 to 2010, several retrospective studies have emphasized the response in terms of clinical symptoms, endoscopic images and histopathology of VTQDBCAT patients to treatment. PPI treatment.
By 2011, the first prospective study with a large number of patients recorded a response rate to PP after 8 weeks of treatment of 50%, of which the histopathological response rate was 80%.
Subsequent to this, several studies and randomized controlled trials continued to demonstrate response rates to PPIs ranging from 33 to 36% with histopathological response rates defined as when the number of BCAT is from 5-7 microfield cells.
A meta-analysis of 33 studies with 619 patients showed a histopathological response rate (<15 BCAT/field) of 50.5% and symptom improvement of 60.8%. There was no difference in patient age and PPI type used, but twice-daily dosing results in better response than once-daily dosing so the recommended dose in adults is for example for omeprazole dosed 20-40 mg twice daily or equivalent.
Time to use PPI for later reevaluation is 8 weeks. Upon discontinuation of treatment, clinical symptoms or esophageal elevations of BCAT may reappear after 3-6 months.
However, the best long-term treatment or maintenance dose is still not much data, so in clinical practice, many doctors choose the solution to use the lowest maintenance dose. effective treatment. A multicenter study of 75 adult PPI-treated patients showed that all patients who abruptly stopped taking PPIs experienced both clinical and histopathological relapses.
The majority of patients will maintain a response for at least one year with gradual reductions to the minimum effective PPI dose. In some patients, when the dose is reduced, there is a relapse, and the dose is increased again. Follow-up data for more than 1 year are not available.

Sử dụng thuốc ức chế bơm proton (PPI) trong điều trị viêm thực quản bạch cầu ái toan
3.2. Systemic steroids In the pathogenesis of VTQDBCAT, inflammatory mediators from BCAT activation play a central role in the formation of lesions on the esophageal mucosa leading to chronic inflammation. The use of corticosteroids in the treatment of conditions or inflammation caused by elevated BCAT has been shown to be effective in a variety of conditions. Liacouras et al. were the first to confirm the efficacy of systemic steroid therapy in pediatric patients with VTQDBCAT and subsequently began to have adult data demonstrating efficacy.
However, when stopping use, the patient will relapse, leading to long-term use with a series of unwanted effects. The 2007 consensus recommended that systemic corticosteroids should be used only in patients requiring rapid relief of acute symptoms such as severe dysphagia, significant weight loss, and esophageal stricture at risk of perforation during dilation. The dose used is 1-2mg/kg/day with a maximum dose of 60mg/day, then gradually reduce the dose.
However, by the 2017 consensus of the American Gastroenterology Association, systemic steroids are no longer recommended in the treatment of the skin as effective as topical steroids while the adverse effects are much greater.
3.3. Topical Steroids To date, there have been numerous randomized controlled clinical trials in both children and adults demonstrating the efficacy of topical steroid use both histopathologically and in clinical improvement. . Fluticasone or budesonide can be used for 2-12 weeks by inhalation or by oral tablet or suspension form.
The 2017 consensus established a recommended dose for use at the start of treatment or to maintain response for both adults and children. When using inhalation, instruct the patient to hold their breath.
Patients should fast for at least 30 - 60 minutes after using the drug to limit the drug drift into the stomach. In terms of adverse effects, so far, only Candida infection has been mainly recorded with the rate of less than 10% and there is no difference in this rate between the inhaled or oral groups.

Người bệnh nên đến gặp bác sĩ để được thăm khám điều trị kịp thời
3.4. Other drugs To date, there are not many data on the efficacy of azathioprine and mercaptopurine in the treatment of VTQDBCAT. Several antiallergic agents used in the treatment of allergic rhinitis and asthma have not demonstrated an improvement in clinical symptoms and histopathology in patients with VTQDBCAT.Montelukast, a leukotriene D4 receptor antagonist may help There was no improvement in symptoms, but no histopathological improvement was achieved and remission was not maintained with discontinuation of topical steroids. Biologic drugs such as anti-IL5 antibodies (mepolizumab, reslizumab), anti-lgE antibodies, anti-TNFα have not shown any real effect on both clinical and histopathological responses.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
References:
Dao Van Long, Dao Viet Hang. Autoimmune diseases of the gastrointestinal tract. Medical Publishing House. Lucendo AJ, Molina - Infante J, Arias Asia et al (2017). Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J,5(3): 335-58. Kinoshita Y, Ishimura N, Oshima N et al (2015). Systematic review: Eosinophilic esophagitis in Asian countries. World J Gastroenterol, 21 (27): 8433-40. Strammann A, Bussmann C, Zuber M, Vanndni S, Simon HU, Schoepfer A. Eo-semophilic esophagitis:analysis of food impection and perforation in 251 adolescent and adult patien clin Gastroen – terol Hepatol 2008; 6:598-600.