This is an automatically translated article.
The article is written by Master - Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital.Gastroesophageal reflux disease (GERD) is the most common cause of noncardiac chest pain. This condition, also known as acid reflux, causes 22 to 66% of noncardiac chest pain attacks. Other, less common esophageal problems that can cause chest pain include muscle problems, also known as esophageal motility disorders.
1. Distinguish chest pain caused by gastroesophageal reflux from chest pain caused by heart
Noncardiac chest pain caused by gastroesophageal reflux disease may be relieved with high dose antisecretory drugs. Gastroesophageal reflux chest pain is often associated with meals and is difficult to distinguish from cardiac chest pain. Certain risk factors for coronary heart disease; such as smoking, obesity and diabetes, etc. are also risk factors for esophageal abnormalities and gastroesophageal reflux disease, complicating the differential diagnosis.Coronary artery disease and gastroesophageal reflux disease can also coexist and their prevalence increases with increasing age. Epidemiological data suggest that 50% of patients with coronary artery disease have experienced one or more typical symptoms of GERD. In contrast, one-third to one-half of patients present with severe chest pain with no evidence of coronary artery disease after invasive examination.
Although difficult, there are ways to distinguish GERD chest pain from cardiac chest pain. As for the location of the pain, both GERD and cardiac chest pain occur in the center of the chest (behind the breastbone). However, cardiac chest pain can spread to the entire chest and other parts of the body. Meanwhile, chest pain caused by gastroesophageal reflux often tends to be local and not spread to other areas. The sensation of pain is also a way to differentiate cardiac chest pain from GERD. When having chest pain due to heart, the patient feels like his chest is heavy, chest tightness, chest is squeezed, ... But with chest pain caused by gastroesophageal reflux, the patient may feel a burning sensation. mid chest area, especially right after eating; persistent heartburn; sore throat;...
However, based on the usual symptoms and medical history, it is still quite difficult for the doctor to confirm whether you have chest pain due to heart or not. You should go to the hospital or medical center to be examined, diagnosed and do some necessary tests to properly determine your condition.
2. It is necessary to distinguish functional chest pain from chest pain related to gastroesophageal reflux disease
Functional chest pain should be differentiated from chest pain associated with gastroesophageal reflux disease. ROME IV-classified functional chest pain defined as posterior chest pain or discomfort, with no esophageal symptoms, and no evidence of gastroesophageal reflux disease, esophageal motility disorder, or esophagitis eosinophils (EoE). Suspected mechanisms include abnormal physical and mechanical properties of the esophagus, esophageal hypersensitivity, dysregulation of autonomic regulation, and altered central processing of esophageal stimuli.
Đau ngực do trào ngược dạ dày thực quản có thể giảm bớt khi dùng thuốc.
3. Treatment of chest pain associated with gastroesophageal reflux disease
The pharmacological treatment of GERD-associated chest pain is complex and still under investigation. The cornerstones of pharmacological treatment are PPIs and H2 blockers, the former considered as primary first-line therapy. Between 78 and 92% of patients with diagnosed gastroesophageal reflux disease (endoscopic findings and/or abnormal pH tests) who received antireflux therapy had improved symptoms.Approximately 10 - 14% of patients with noncardiac chest pain who respond to PPI therapy do not have GERD. The duration of PPI therapy is not clear, however, a course of 2 to 3 months is generally recommended. If there is no response to the PPI trial within 2 weeks, PPI therapy should be discontinued. In a recent meta-analysis, PPI treatment in patients with noncardiac chest pain associated with GERD was more effective than placebo.
While outcomes in patients with noncardiac chest pain without GERD are inconsistent. In an uncontrolled trial, 2 weeks of high-dose rabeprazole (40 mg) improved symptoms in 81% of patients with noncardiac chest pain with gastroesophageal reflux disease. Currently, a full course of double-dose PPIs (during 2 months) is still considered the best initial treatment for patients with GERD-associated noncardiac chest pain. .
4. The role of surgery
Laparoscopic fundoplication (Nissen fundoplication) is a surgical technique that restores the anti-reflux barrier by enhancing basal pressure at the gastroesophageal junction, repairing diaphragmatic hernia, and strengthening peristaltic function of the esophagus. Both total and partial reconstruction of gastric aneurysms are performed in patients with noncardiac chest pain associated with gastroesophageal reflux disease.81 – 96% of those with reflux-related symptoms had improved symptoms after surgery compared with those with no correlation. Surgery to create an antireflux valve has been shown to be more effective in patients with typical GERD symptoms associated with noncardiac chest pain and in those who respond to therapy. PPI therapy compared with those with atypical presentation of the disease and low response to PPIs.
Some issues to watch out for after surgery: This effective procedure has some side effects such as the oesophageal junction is significantly changed after surgery leading to more frequent peristaltic disturbances, increased pressure on swallowing and dysphagia after surgery. Postoperative dysphagia may affect up to 90% of postoperative patients with varying degrees of severity (classified on a four-point Likert-like scale).
Endoscopic gastric aneurysm reconstruction is currently the "gold standard" technique for the surgical treatment of gastroesophageal reflux disease. However, it is indicated only when an optimal dose of a PPI does not control the disease or long-term medical therapy is not possible.
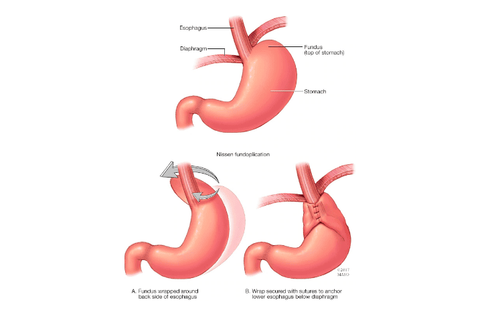
Phẫu thuật tạo hình phình vị dạ dày trong điều trị trào ngược: Tạo ra một van nhân tạo ở chỗ nối thực quản dạ dày.
5. Treatment of chest pain caused by hypersensitivity of the esophageal mucosa
When chest pain is caused by esophageal mucosal hypersensitivity, recommended treatment includes visceral pain modifiers such as tricyclic antidepressants (TCAs), trazodone, adenosine antagonists, serotonin reuptake inhibitors. -norepinephrine (SNRI) and selective serotonin reuptake inhibitors (SSRIs). Although trials evaluating pain modifiers are small and often not placebo-controlled, these drugs remain the mainstay of treatment for esophageal hypersensitivity. Among them, venlafaxine and sertraline have shown the most encouraging data for pain relief in patients with noncardiac chest pain.6. Treatment of non-cardiac chest pain and psychological disorders
Given the association between noncardiac chest pain and psychological disturbances, cognitive behavioral therapy has been investigated as a possible intervention. Demiryoguran et al. found that: Patients who underwent cognitive behavioral therapy significantly reduced the number of days with chest pain, severity of symptoms, psychological stress, decreased pain activity and depressed mood compared with the control group. However, further investigation is needed before recommending routine cognitive behavioral therapy for the treatment of noncardiac chest pain. Cognitive behavioral therapy should also be considered in patients with high levels of mental instability and frequent anxiety.6. Conclusion
Diagnostic tools for extraesophageal reflux disease:| Công cụ chẩn đoán | Khuyên dùng |
| Nội soi thực quản dạ dày | Được đề xuất nếu xuất hiện các triệu chứng báo động (giảm cân, tuổi > 50, thiếu máu). |
| Theo dõi pH thực quản trong 24 giờ | Khuyên dùng cho ho mãn tính, hen suyễn, viêm thanh quản, tổn thương khoang miệng, đau ngực không do tim, viêm phổi hít. |
| Đo trở kháng pH | Khuyên dùng cho bệnh hen suyễn, viêm thanh quản. |
| Dùng thuốc kháng tiết axit PPIs | Khuyên dùng cho ho mãn tính, hen suyễn, viêm phổi hít do viêm thanh quản, tổn thương khoang miệng. |
| Nội soi thanh quản | Khuyên dùng cho bệnh viêm thanh quản. |
| Nội soi phế quản | Khuyên dùng cho bệnh ho mãn tính. |
Lifestyle changes; such as elevating the head of the bed, losing weight, stopping smoking, and making dietary changes (reduced fat, chocolate, alcohol, citrus, tomatoes, coffee and tea, avoiding large meals and eating) three hours before bedtime) is always recommended, both in typical gastroesophageal reflux disease and associated extraesophageal manifestations.
Pharmacotherapy is used in all forms of gastroesophageal reflux disease. This therapy is particularly effective in patients with evidence of acid reflux requiring pH monitoring. H2 blockers are not superior to PPIs but can be used as a reasonable alternative. In some difficult-to-treat cases, both PPIs and H2 blockers can be combined. Antireflux surgery may be used in noncardiac chest pain or chronic cough with acid reflux-related manifestations to monitor pH in patients who are responsive but dependent on PPI therapy.
To prevent the risk and promptly treat chest pain due to gastroesophageal reflux or chest pain due to other causes, please make an appointment with Vinmec Health System Hospitals nationwide to receive treatment. Best Service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.