This is an automatically translated article.
The article is written by Dr. BS Mai Vien Phuong - Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital.
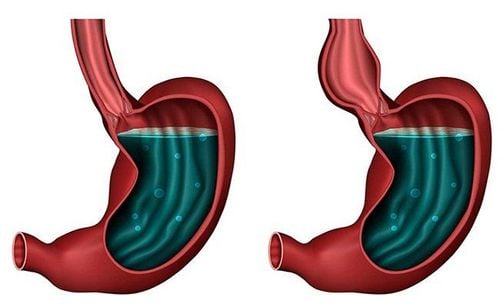
Achalasia is a functional disorder in which the esophagus is not able to push food down into the stomach (abnormal peristalsis) and the lower esophageal sphincter opens incompletely (hypertension). lower sphincter) causing stagnation of food in the esophagus.
1. What is an overview of cardiac spasms?
Cardiac spasm is a disease with an obstruction of the esophageal outlet associated with esophageal motility disorders, making the patient difficult to digest.
Symptoms of achalasia in the early stages are that the patient sometimes feels heaviness in the chest due to gastroesophageal reflux disease, choking on solid and liquid foods, then increasing choking. gradually accompanied by vomiting after eating. If the disease is left for a long time and is not treated in time, the disease will cause loss of work capacity and weight loss. Although it is a benign disease, it adversely affects health and reduces quality of life.
To date, the exact cause of cardiac spasm has not been determined. Previously, achalasia was treated by two methods: endocardial balloon dilatation or Heller surgery to open the myocardium. The limitation of these methods is the risk of complications.
2. Technique of opening the mouth muscle to treat cardiac spasms
Instead of opening the muscle through the abdomen like the Heller surgery, with the oral technique, the patient will not have any incision in the abdomen. Oral endoscopic myocardiocentesis (POEM) is a new method to treat cardiac spasms with high efficiency
The advantage of POEM is opening the oesophagogastric muscle by oral flexible endoscope...Open Oral endoscopy (POEM) has been developed as an effective and minimally invasive endoscopic treatment.
POEM technique is now widely described in many places. After endotracheal anesthesia and intravenous antibiotics, the endoscopist will identify the lower esophageal sphincter (LES) and inflate the submucosa in the middle oesophagus with a staining solution (to define the border). boundaries between muscle layers). The scope is inserted into the submucosa through a longitudinal incision with an electric knife, and creates a long tunnel in the submucosa through the lower esophageal sphincter to the cardia of the stomach, exposing the entire muscle. inner ring (Figure 1). Then, muscle dilation is performed starting from a point a few centimeters from the original incision, usually 8-10 cm above the gastroesophageal junction and down to the gastrogastric region 2-3 cm. The sphincter bundle was identified and muscle resection was performed, so that the lower esophagus would dilate.

Người bệnh được tiến hành gây mê nội khí quả trước khi thực hiện kỹ thuật POEM
2.1 Instruments used in the POEM procedure The 9.8 mm outer diameter straight bronchoscope (GIF-H260; Olympus, Tokyo) commonly used for upper gastrointestinal endoscopy will have a cap attached (MH-588, Olympus) at the tip. A triangulated electric knife (KD-640L; Olympus) was used for submucosal resection and sphincterectomy. A hemostatic device (Coagrasper, FD-411QR; Olympus) is used to cauterize the great vessels before cutting and to stop bleeding. CO2 was injected during the procedure using a CO2 pump (UCR; Olympus). The VIO 300D generator is used for surgical instruments and hemoclips (EZ-CLIP, HX-110QR; Olympus) are used to close the submucosal entry incision.
2.2 Procedure for performing the POEM procedure The patient is under general anesthesia with positive pressure ventilation and a pressure higher than that produced by the injected CO. The UCR CO2 pump (Olympus) is used with a regular pump tube (MAJ-1742; Olympus), which helps maintain a constant CO2 injection rate of 1.2 liters/min.
Submucous tunneling: The entry to the submucosa is made in the middle esophagus, about 13cm above the gastroesophageal junction (GEJ). 10 ml of physiological saline solution mixed with 0.3% indigo carmine was injected into the submucosa. Make an incision along the mucosal surface about 2cm to create a path into the submucosa (using dry cut mode, 50W, effect 3) Then, endoscopic submucosal dissection (ESD: Endoscopic submucosal dissection) is applied to Create a downward tunnel, through the GEJ, into the stomach about 3 cm. The width of the submucosal tunnel is about 1⁄2 of the esophageal lumen. Spray coagulation mode (50W, effect 2) is used to remove the submucosa. Large vessels were held by hemostatic forceps in soft coagulation mode (80W, effect 5). Sphincterotomy: Sphincterotomy started at 3cm below the incision, about 7cm above the GEJ. Using the tip of the electric knife, the triangle tip captures the sphincter and lifts the muscle toward the lumen of the esophagus. Cut muscle with spray coagulation mode (50W, effect 2). Continue the myotomy from the esophagus to the stomach until the scope passes through the narrowing of the lower LES (Figure 2d). When the tip of the scope reaches the stomach, the submucosa will suddenly become wider. Continue to cut the muscle about 2cm more towards the stomach. After the sphincter bundles have been resected, locate the longitudinal bundles beyond the confines in the area of resection. Complete resection of the sphincter bundles was verified endoscopically. Gastroscopy after complete resection of the sphincter showed smooth circulation of the laparoscope through the GEJ with little resistance. Closing the mucosal opening: The 2cm inlet of the mucosa was closed with 5 hemostatic clips. Successful access closure is verified endoscopically. At the end of the procedure, gastroscopy re-examined the flexible circulation of the scope through the GEJ. 2.3 Post-procedural examination Check for bleeding, perforation, tearing of esophageal mucosa, results of cardiac dilation. Absorb all the fluid and gas in the stomach. A solution of 20ml of physiological saline mixed with 80mg of Gentamycin is sprayed into the mucosal tunnel before closing the mucosa. Close the mucosal opening with the distal to proximal endoclip. C-arm scan of the chest and abdomen after the procedure to evaluate the air status in the thoracic cavity, mediastinum, peritoneal cavity.. Currently, the results from the meta-analyses show a success rate of 80 to 100%.

Sau thủ thuật, người bệnh được kiếm tra bằng máy chụp C-arm vùng ngực
2.4 Monitor during technique Monitor vital signs Follow guidewire path Monitor abdominal free air. 2.5 Monitoring for complications Early complications can be:
Perforation 0-12.8% Pneumomediastinum>10% Pneumoperitoneum>10% Pneumothorax: <1% Severe pain after POEM: 10 % Peritonitis Reflux esophagitis: 20-46% Pain 0-7.4% Bleeding 7% Currently, over 1000 cases of POEM have been performed in the world. this art.
2.6 Care after the procedure The first day after the procedure:
Clinical examination of the chest and abdomen. Complete blood cell analysis. Chest radiograph, esophagogastroduodenoscopy, esophageal radiograph with baryt. If there are no signs of mucosal damage, open the esophageal sphincter: the patient drinks milk, eats diluted porridge.
2nd day after procedure: patient can eat soft foods
3rd day: eat normal diet again

Sau khi thực hiện thủ thuật, ngày đầu tiên người bệnh thực hiện nội soi thực quản dạ dày
2.7 Measures to prevent and manage complications and complications Prevention of perforation of the longitudinal muscle layer or mucosa: Careful submucosal dissection, careful hemostasis to have a clear surgical field, especially during surgery area of gastroesophageal junction Prevention of bleeding complications: stop bleeding carefully.
3. Conclusion
Oral endoscopic myotomy is a new method for the treatment of achalasia. The advantages of this method are minimally invasive procedure, early patient recovery, short hospital stay and few complications.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of doctors, modern equipment and technology, but also stands out for its examination, consulting and service services. comprehensive and professional medical treatment; civilized, polite, safe and sterile medical examination and treatment space.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
LEARN MORE
Advantages of robotic surgery for hernia treatment of abdominal wall hernias Diagnosis and emergency treatment of gastrointestinal bleeding by gastro-oesophageal endoscopy at Vinmec Air balloon dilation to treat cardiac spasms