This is an automatically translated article.
Article by Master, Doctor Le Thai Bao - ICU Doctor - ICU Department - Vinmec Times City International General Hospital.
Intraventricular hemorrhage is an independent risk factor for increased morbidity and mortality in patients with hemorrhagic stroke. The sequelae and death of intraventricular hemorrhage are often the result of complications of ventricular dilation (obstructive ventricular dilatation and circulating ventriculomegaly). The severity of ventricular dilatation is correlated with intraventricular blood volume and the length of time CSF is exposed to intraventricular blood clots.
Intraventricular fibrinolysis is a technique that uses fibrinolytic drugs (rt-PA) injected into the ventricles through ventricular drainage to rapidly dissolve blood clots in the ventricles (especially the 3rd and 4th ventricles). , facilitate early opening of the lower ventricular system and thereby avoid complications of ventricular dilatation.
1. Anatomical landmarks of the ventricular system
The ventricular system consists of a pair of lateral ventricles, each of which is connected to the third ventricle by the foramen of Monro. The third ventricle is connected to the fourth ventricle by the aqueduct of Sylvius.
Three axes from the fourth ventricle, two Luschka lateral foramen and one mid-Magendie foramen, form a system of centrally enlarged and interconnected subarachnoid spaces called cisterns. The posterior fossa cisterns connect to the subarachnoid spaces on the cerebral convexities via small pathways to the occipital leaflets. The basal cisterns connect to the intracranial subarachnoid spaces and spinal cord.
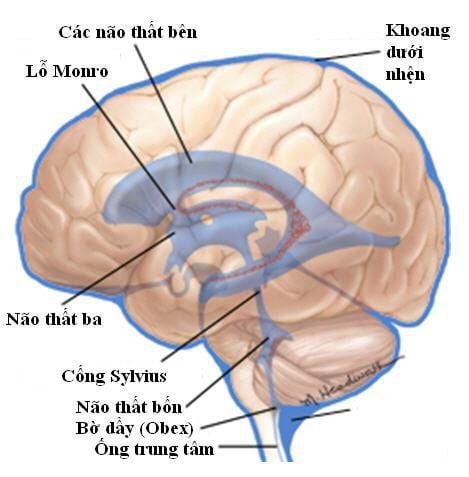
Hệ thống thất não gồm có một cặp não thất bên, mỗi não thất bên kết nối với não thất ba bởi lỗ Monro.
2. Indications for intraventricular fibrinolysis
Intraventricular fibrinolysis is indicated for cases where the following criteria are met:
Sudden disturbance of consciousness. Intracerebral and/or intraventricular hemorrhage. Cerebral parenchymal hematoma volume ≤ 30 mm3 (volume of hematoma calculated according to ABC/2 formula). Bleeding into the 3rd and/or 4th ventricles. Acute obstructive ventricular dilatation and ventricular drainage have been performed. No further intracerebral and/or intraventricular hemorrhage, no new bleeding (bleeding around the ventricular drain leg) after 6 hours of ventricular drainage. Systolic blood pressure < 200 mmHg for at least 6 hours before performing ventricular fibrinolysis.
3. Contraindications to intraventricular fibrinolysis
Intraventricular fibrinolysis is contraindicated in one of the following cases:
ruptured cerebral aneurysm, ruptured cerebral arteriovenous malformation or brain tumor. Vascular malformation in choroid plexus or Moyamoya syndrome. Coagulopathy (platelet count < 100,000; INR > 1.4). Pregnant. Subtentorial cerebral hemorrhage (brainstem hemorrhage or 3rd cranial nerve palsy). Subarachnoid hemorrhage. Further progressive intracerebral and/or intraventricular hemorrhage. Visceral bleeding. Bleeding under the skin. The patient and/or the patient's family does not agree to perform the technique.

Tiêu sợi huyết não thất chống chỉ định với phụ nữ có thai và một số trường hợp khác.
4. Preparation steps
Practitioner : 1 physician trained in ventricular drainage techniques and the use of thrombolytics and 2 surgeons trained in assisting the physician with ventricular drainage and fibrinolysis blood. Instruments: fibrinolytic drug rtPA or Alteplase (brand name is Actilyse ® of Boehringer Ingelheim company, fully qualified and licensed to use by the Ministry of Health, close 50mg alteplase tube and 50ml distilled water for medicine). Medicine: topical antiseptic, usually using Povidone iodine 10% (Betadine). Physiological saline solution (NaCl 0.9%) bottled sterile. Sterile 5ml and 10ml syringes, sterile needles. Sterile dressings, sterile gloves, sterile gasoline and sterile gown. Monitor (monitor) and monitor intracranial pressure. Patients: Need to check vital functions (pulse, blood pressure,...), intracranial pressure. Examination to assess the state of consciousness, neurological damage, signs of pupil size and reflexes,... Status of ventricular drainage, cerebrospinal fluid (quantity, nature of cerebrospinal fluid, .. .) Re-examine the CT scans of the brain, MSCT of the brain vessels to re-evaluate the state of cerebral hemorrhage, intraventricular bleeding, etc. The patient or family member must record a commitment to the technique.
5. Steps to conduct intraventricular fibrinolysis
Check records: Check indications, contraindications and commitment to agree to perform the procedure. Check the patient: Check the patient's vital functions before the procedure. Perform ventricular drainage technique: Ventricular drainage is indicated to monitor and control intracranial pressure and treat acute ventricular dilatation. Ventricular drainage was placed in the frontal horn of the lateral ventricle with the least bleeding (the site of ventricular drainage was re-checked by cranial CT). For resuscitation to protect the airways with endotracheal intubation, artificial ventilation if coma is deep (GCS < 8). Sedation and analgesia are appropriate with midazolam and/or fentanyl.
Intracranial pressure is continuously monitored and treated if ICP increases ≥ 20 mmHg in 5 minutes. Blood pressure is monitored regularly, preferably by continuous monitoring.
Arterial catheterization and treatment if mean blood pressure ≥ 120 mmHg. Extubation when GCS > 8 and brainstem reflexes are satisfactory. In case of prolonged artificial ventilation and difficult to wean from mechanical ventilation, conduct tracheostomy after 5 days of intubation. Biochemical tests are performed daily to monitor liver, kidney, and electrolyte function.
6. Intraventricular fibrinolysis technique
Operations to perform intraventricular fibrinolysis must be absolutely sterile and are carried out according to the following steps:
Wear a sterile gown, wear sterile gloves, disinfect the injection site (fork) 3 on ventricular drainage) with povidine iodine 10%, with sterile dressings. Use a sterile syringe to aspirate 6 ml of cerebrospinal fluid through the ventricular drain. Inject 1 mg of rt-PA in a sterile syringe into the ventricles through ventricular drainage. Using a sterile syringe, inject 5ml of physiological saline into the ventricles through ventricular drainage. Close the ventricular drainage system for 2 hours, during which time intracranial pressure is continuously monitored. If the intracranial pressure rises above 20 mmHg for more than 5 minutes without any stimulation to the patient, treat the raised intracranial pressure with intravenous mannitol infusion, increasing ventilation (if the patient is artificially ventilated). If intracranial pressure still increases after the above treatments, open the ventricular drainage system to drain the CSF out. If intracranial pressure remains elevated after opening of the ventricular drainage system, an emergency cranial CT scan should be performed to rule out bleeding complications. After 2 hours, close the ventricular drainage system, open the ventricular drainage system to drain the cerebrospinal fluid out. Brain CT scans were taken after 24, 48, and 72 hours. Thrombolytic agents (rtPA) are injected into the ventricles every 8 hours until the blood in the third and fourth ventricles is depleted for a maximum total dose of ≤ 9 mg.
7. Track progress
Closely monitor vital indicators, state of consciousness, pulse, blood pressure, electrocardiogram, respiratory status.
Monitoring the progress and results of the technique: Clinical changes (Glasgow), electrocardiogram, results of ventricular revascularization, intracranial pressure, respiratory status, blood pressure,...
Monitoring complications of fibrinolytic drugs: Bleeding at injection site, catheter foot, bleeding under the skin, altered consciousness (cerebral hemorrhage), hematuria, gastrointestinal bleeding,...

Theo dõi sát các chỉ số sinh tồn, tình trạng ý thức, mạch, huyết áp, điện tim, tình trạng hô hấp.
8. Possible complications and complications during treatment
New cerebral and/or intraventricular hemorrhage. Cerebral parenchymal hematoma and/or progressive (recurrent) intraventricular hemorrhage. Hemorrhage around the leg draining the ventricles. Central nervous system infection. Encephalitis, meningitis. Subarachnoid brain abscess. Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading doctors, modern equipment and technology, but also stands out for its examination and consulting services. and comprehensive, professional treatment, civilized, polite, safe and sterile medical examination and treatment space. Therefore, when having health problems, customers can go to the hospital for advice and treatment instructions to bring the best results.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.