This is an automatically translated article.
Article written by Doctor of Urology Department, Vinmec Central Park International General Hospital
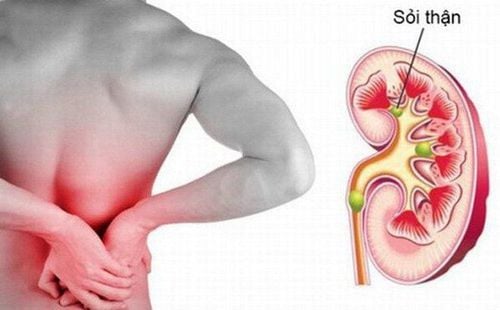
Kidney stones are a common disease of the urinary system. Currently, there are many advanced surgical methods for non-invasive lithotripsy. Depending on the patient's condition and the size of the stone, the doctor will prescribe the appropriate treatment method.
1. Overview of surgical treatment of kidney stones
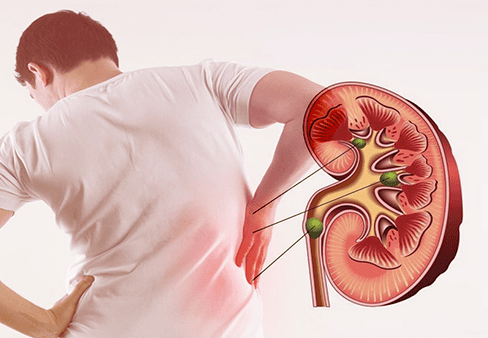
Kidney stones are a common disease of the urinary system. In the United States, about 10 to 15% of the population suffers from this disease [Norlin et al, 1976, Johnson et al, 1979]. The frequency of the disease in Vietnam is unknown. However, the frequency of the disease may be higher because Vietnam is located in a geographical area with many favorable factors for stone formation such as: hot and humid climate, geology, calcium-rich water sources...
Since ancient times Recently, Hippocrates discovered the presence of stones in the kidney. He was also the first to describe renal colic and the technique of perirenal abscess drainage. Over the centuries, Cardan (1550) reported a case of incisional resection of a back abscess in a young female patient that removed 18 stones [Denos, 1972].
Over the next two centuries, most surgeons removed stones only in cases of septic, pus-filled, or palpable stones in the kidney. Since the 19th century, many advances in kidney stone surgery have been reported. In 1879, Heineke popularized the technique of opening the renal pelvis to remove stones. Josep Hyrtl (1892) and Max Brodel (1902) describe the avascular plane near the midline of the renal curvature (5mm posterior to the kidney).
Although the avascular route is an important invention, bleeding in kidney stone surgery is still a difficult problem and causes many difficulties in surgery. Many authors have proposed solutions to control bleeding during surgery such as vascular insertion of the renal hilum or suture of renal tissue (Creny, 1987) but the results are still not satisfactory.
Sỏi thận là bệnh phổ biến ở hệ tiết niệu
In 1965, Gil-Vernet was the pioneer in performing extensive stone removal surgery in the renal sinus. This technique is considered an important advance in open stone surgery. In 1968, Smith and Boyce presented the technique of anatrophic nephrolithotomy to remove coral stones.
Although new surgical methods give quite impressive results, high stone clearance rate but damage many renal tissue owners and therefore new techniques and technologies continue to be researched.
Recently, many important advances in the fields of: bronchoscopes, X-ray imaging and lithotripsy devices (pulse, ultrasound, hydroelectric and laser) have dramatically changed methods. Surgical treatment of kidney stones. As a result, there are many less invasive techniques used in the treatment of kidney stones such as: extracorporeal lithotripsy, percutaneous renal stone removal, endoscopic retrograde lithotripsy...
The main goal of surgical treatment Kidney stones are achieving the highest possible stone clearance rate with minimal complications and kidney damage. Since the advent of extracorporeal lithotripsy and advances in urological endoscopy, most patients with kidney stones have been treated with minimally invasive methods. These techniques are effective and cause less damage to the host kidney tissue than open surgery.
When there are many treatment options, there are also many inconsistent opinions about indications and treatment methods. In many cases, choosing an optimal treatment for a patient is a challenge for the urological surgeon. Before treatment, the patient needs to be fully evaluated for related factors to come up with an appropriate treatment solution. The characteristics of the stone are one of the important factors determining the treatment method, including the number and size of the stones (stone burden) and the location of the stones (Motola and Smith 1990). Factors related to the anatomical features of the kidney also play an important role, such as: obstruction, hydronephrosis, anastomosis, calyx diverticulum and abnormalities in the position and number of the kidneys. In addition, the patient's clinical characteristics must also be carefully evaluated such as urinary tract infection, obesity, coagulation disorders ...
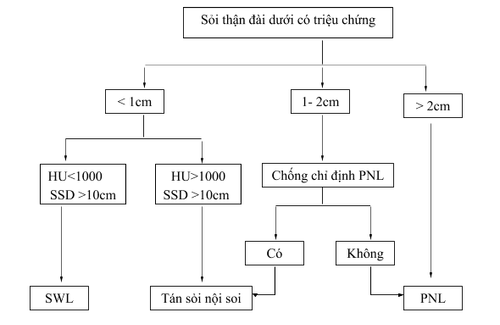
Figure: Diagram of treatment of kidney stones other than lower calyces
![HU: đơn vị Hounsfield, SSD: khoảng cách từ da đến sỏi thận (Nguồn: Wen CC, Nakada SI. Treatment selection and outcomes: renal caculi. Urol Clin North Am 2007; 34[3]:409-19)](/static/uploads/small_20200629_020954_411805_screenshot_15933965_max_1800x1800_png_f65e00944d.png)
HU: đơn vị Hounsfield, SSD: khoảng cách từ da đến sỏi thận (Nguồn: Wen CC, Nakada SI. Treatment selection and outcomes: renal caculi. Urol Clin North Am 2007; 34[3]:409-19)
Lower calyx stones
Picture: Diagram of treatment of lower calyx stones
Nguồn: Galvin GJ, Pearle MS. The contemporary management renal and ureteric calculi. BJU Int 2006; 98:1283-8
2. The surgical treatment of kidney stones
2.1 Lithotripsy outside the body
Most patients with simple kidney stones, less than 2cm in size, can be effectively treated with extracorporeal lithotripsy. This is a minimally invasive treatment with an acceptable success rate. The rate of gravel removal varies depending on the size of the gravel. The larger the stone, the lower the success rate. However, this is the least invasive treatment method and is considered the first choice among the current methods of treating kidney stones.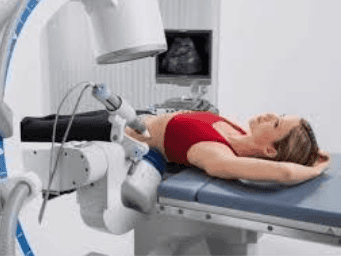
Tán sỏi ngoài cơ thể là phương pháp điều trị an toàn và tỷ lệ sạch sỏi cao
When extracorporeal lithotripsy does not achieve the desired effect, retrograde endoscopic lithotripsy or PNL are alternatives to consider. Factors associated with low stone clearance rate such as large stone size, obstructing stone, hard stone composition, obesity or physical deformity. The weighted mean stone clearance rate with extracorporeal lithotripsy was 66.7%.
Table of results of treatment of extracorporeal lithotripsy
| Nghiên cứu | Máy tán sỏi | Số lượng bệnh nhân |
Kích thước sỏi trung bình |
Tỉ lệ sạch sỏi (%) |
| Albala et al, 2005 | Medstone STS-T | 326 | 8.2 mm | 53 |
| Jain et al, 2004 | LithoTron | 298 | 8 mm | 66 |
| Johnson et al, 2003 | DoLi S | 176 | 9.7 mm | 73 |
| Portis et al, 2003 | HM3 | 38 | 9.6 mm | 79 |
| LithoTron | 38 | 9.9 mm | 58 | |
| Sorensen et al, 2002 | DoLi U50 | 42 (an thần tĩnh mạch) | <10 mm (8.1) | 55 |
| 89 (gây mê) | <10 mm (7.3) | 88 | ||
| 18 (an thần tĩnh mạch) | 11-20 mm (15.0) | 56 | ||
| 37 (gây mê) | 11-20 mm (14.4) | 84 | ||
| Matin et al, 2001 | MFL 5000 | 356 | 103 mm2 | 77 |
| Modulith SLX | 173 | 71 mm2 | 67 | |
| Fallon et al, 2000 | MFL 5000 | 105 | 70% < 10 mm | 47 |
2.2 Retrograde endoscopic lithotripsy
In 1983, Huffman was the first to describe the technique of lithotripsy with a rigid ureteroscope, which uses ultrasound energy to dissolve stones. The use of rigid bronchoscope faces many difficulties due to limited access to the renal calyces, difficult to observe the whole pyelonephritis system, especially the lower renal calyces. However, this approach has opened up a new potential for the natural treatment of kidney stones.
About 2 decades later, when flexible ureteroscopes were introduced, access to stones improved. The bronchoscope can be moved flexibly to reach every taste of the excretory system. This is an important advancement that is increasingly being used in the treatment of upper urinary tract stones with a high probability of success.
In 1990, Fuchs reported in a study done on a large number of patients with kidney stones. The author performed retrograde lithotripsy with a flexible bronchoscope 1 to 2 weeks after catheterization of the ureter. The stone removal rate was 87%, higher than some other treatment methods at that time. In this study, the complication rate was low, only 2 cases of urinary tract infection after lithotripsy.
Tán sỏi nội soi ngược dòng
With increasingly sophisticated manufacturing technology of bronchoscopes and lithotripsy instruments, surgery has been facilitated. Upper urinary tract stones become accessible with the small bronchoscope and thus can access kidney stones located even in hard-to-reach locations such as the lower calyx (Lucasewycz, 2004; Pearl, 2005).
Many studies with large numbers of patients confirm the role of this treatment with the prospect of increasing popularity. The outcome of treatment in the first successful lithotripsy ranges from 70 to 80% (Mariani, 2007; Breda, 2008). With cases of second lithotripsy, the complication rate is also very low, the most common are fever and urinary tract infection.
However, this method is not indicated for large kidney stones. Although not widely used, there are some doctors who have successfully performed retrograde lithotripsy in some patients with coral stones (Mariani 2007).
2.3 Laparoscopic surgery
Technological advances in laparoscopic surgery provide yet another potential means of application in the treatment of kidney stones. However, laparoscopic or retroperitoneal approaches are indicated when the expected outcome of treatment with extracorporeal lithotripsy or retrograde endoscopic lithotripsy has a low probability of success.
In some cases, laparoscopic stone removal is considered reasonable and safe. These are the situations of kidney stones associated with anastomosis, stones located in the diverticulum or hydronephrosis with thin tissue dilatation, extra-sinus pyelonephritis ...
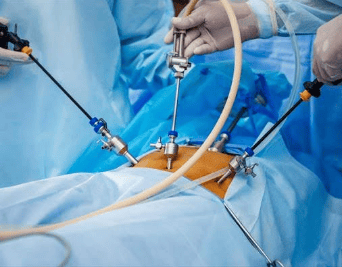
Phẫu thuật nội soi
In addition to these cases, laparoscopic kidney stone removal is still very limited and does not achieve the expected benefit. According to Dasai and Asimo (2008), only about 1% of patients are treated with this method. The most common indication in this study group is kidney stones associated with pyelonephritis - ureteral junction disease.
2.4 Open surgery for kidney stones
Previously, most patients with symptomatic kidney stones had to undergo open surgery to remove the stones. Patients with small-to-moderate stones underwent pyelonephritis or nephrostomy to remove stones. Large stones, complex kidney stones, or coral stones require more complex techniques such as anatrophic nephrolithotomy, pyelonephritis combined with aortic dissection or stone removal. and autologous kidney transplant.
However, with extracorporeal lithotripsy and endoscopic treatments with many outstanding advantages, the role of open surgery has been significantly reduced in the treatment of kidney stones. Currently, open surgery is the least common indication for treatment of upper urinary tract stones, and is the last choice when other treatment measures do not bring the expected effect.
Matlaga and Assimo (2002) statistics, only 0.7% of open surgery cases in 986 surgeries between 1998 and 2001. However, open surgery is still necessary in patients with complicated kidney stones. In the calculus consensus conference, including partial and total gallstones, the recommended initial treatment is PNL or PNL in combination with extracorporeal lithotripsy. Open laparotomy is an alternative if repeated percutaneous or endoscopic interventions are required to remove stones.
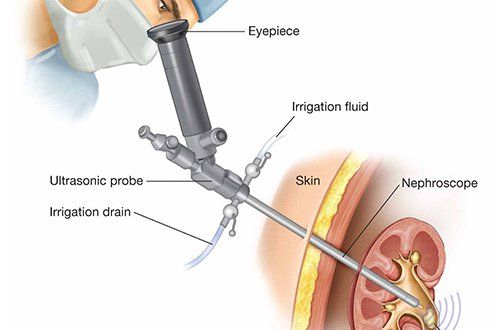
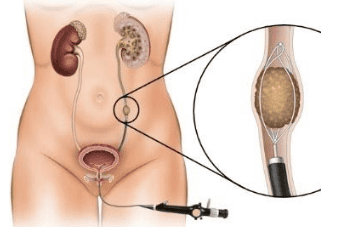
2.5 Percutaneous kidney stone removal
Fennstrom and Johansson were the first to describe the technique of tunneling into the kidney for stone removal in 1976. Subsequent studies have shown that PNL is a routine technique in the treatment of patients with large stones. and complex (Alken, 1981; Segura, 1982; Clayman, 1984).
Advances in techniques as well as new technologies make it easier and more convenient for urological surgeons to remove kidney stones through the skin. Because of the better therapeutic effects than open surgery, PNL gradually replaced open surgery at most centers (Matlaga and Assimos, 2002).
Periodic health check-ups help detect kidney stones early, so that you can have a treatment plan for optimal results. Currently, Vinmec International General Hospital has general health checkup packages suitable for each age, gender and individual needs of customers with a reasonable price policy, including:
Health checkup package general Vip Standard general health checkup package Patient's examination results will be returned to your home. After receiving the results of the general health examination, if you detect diseases that require intensive examination and treatment, you can use services from other specialties at the Hospital with quality treatment and services. outstanding customer service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.