This is an automatically translated article.
Esophageal and tracheal fistula is a congenital malformation acquired in children. This condition is not so common in babies born. The only way to treat the disease is to close the esophageal fistula.1. What is an esophageal fistula?
Tracheoesophageal fistula is a condition in which there is an abnormal connection between the esophagus and the trachea. Normally, the esophagus and trachea are two completely separate tubes. It occurs when the fetus is developing in the mother's womb.
When a baby has an esophageal fistula, gas and fluid can move from tube to tube through the connection site. As a result, children are prone to pneumonia and other problems related to the respiratory and digestive tracts.
Tracheoesophageal fistulas are of three types:
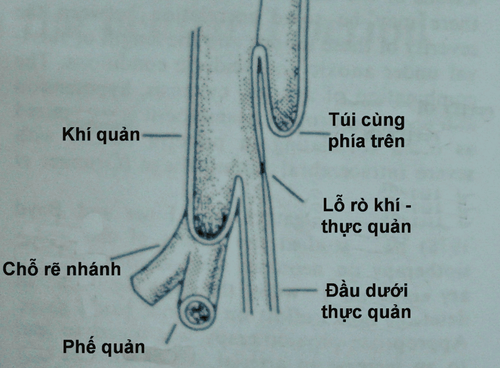
Type 1: The upper part of the esophagus ends in a cul-de-sac and the lower part attaches to the trachea. This type accounts for 80-90%. Type 2: The upper part of the esophagus communicates with the trachea, the lower part ends with a small pouch. Type 3: H-shaped type. The esophagus and trachea are complete and connected by a connecting tube. This type is the rarest and difficult to diagnose because the child is eating and breathing normally. Children with this type are very difficult to overcome.

Rò thực quản khí quản xảy ra khi vị trí nối giữa thực quản và khí quản bất thường
In addition, the tracheoesophageal fistula can be divided into 3 levels as follows:
Grade I: The mucous coating is destroyed. Grade II: Mucous layer, submucosa, and part of the muscle layer are destroyed. Grade III: All layers of the esophagus and surrounding tissues are destroyed. Esophageal-tracheal fistula occurs in neonates with other congenital malformations.
According to research, one out of every 3,000 babies is born with a fistula in the esophagus and trachea. In boys, the incidence is higher. The age of the mother is also proportional to the rate of children with this defect.
2. Common clinical symptoms
Appearance of white foam or bubbles in the mouth. When eating, often cough or choke. Vomit. The skin is pale and blue when the child eats. Shortness of breath Round abdomen, bloating, flatulence. In addition to the above symptoms, your baby may have other signs. Contact your doctor for answers to your questions.
3. Causes of tracheoesophageal fistula
During pregnancy, the fetus is developing and perfecting its organs, including the trachea and esophagus. Initially, the trachea and esophagus develop as two separate tubes. When the fetus is 4-8 weeks pregnant, a septum forms between the esophagus and the trachea. When this septum does not form properly, an esophageal fistula develops.4. How to diagnose esophageal and tracheal fistula?
Esophageal fistula can be diagnosed with an X-ray, which shows air in the intestines.
Also can diagnose by endoscopy. This method is not effective in locating small fistulas.
5. How to treat esophageal fistula?
Children with esophageal and tracheal fistulas need surgery to save their lives. Except in the case of children with H-shaped disorder, they cannot live. However, before surgery, the child should have the following appropriate care:

Rò thực quản khí quản cần phải được phẫu thuật
Keep the child in an elevated position to avoid reflux and aspiration of gastric juices. Regularly suction the baby's mucus and saliva with a tube. A nasogastric tube may be placed. Do not feed children.
6. Surgery to close the esophageal fistula
Before surgery, the patient and family are clearly explained the condition as well as the method of surgery to be performed. In addition, the doctor will also explain about possible complications, complications, sequelae after surgery or due to anesthesia, anesthesia, pain relief or because of the patient's physical condition.
Patients need to fast before surgery and clean the surgical area. Estimated surgery time is 180 minutes.
Steps to perform surgery to close the esophageal fistula:
Put the patient in a 90 ̊ left lateral position, put a pillow under the armpit, and the right hand is placed on a hanger. Disinfect the surgical site and conduct surgery. The incision is in the right posterior position, approximately in the right IV or V intercostal space. To reveal an esophageal fistula, a simple loop ligation is required. After closing the fistula, the tracheal fistula will be sutured with 5.0 vicryl suture, the distance between the stitches is 23mm. Esophageal fistula was sutured with vicryl 4.0 suture along with mediastinal pleural enhancement. Surgery should be performed under the guidance of a nasogastric tube.
7. Possible complications after surgery
Gastrointestinal bleeding : Appears in the first 48 hours or the following days. Bleeding bright red, profuse, through the gastric tube. In addition, the patient may also vomit blood, defecate black, change the general condition (pale, anxious, rapid pulse, low blood pressure). At that time, it is necessary to re-operate to check and stop the bleeding. It is necessary to monitor the condition of the duodenal wall suture or wound infection for timely treatment. Monitor the general condition of the patient such as pneumonia... Infusion: The amount of fluid and the type of fluid depends on the patient's condition. Antibiotics: Prophylactic antibiotics or therapeutic antibiotics can be used as directed by the doctor. Thus, esophageal-tracheal fistula is an uncommon and dangerous anomaly, which can be treated by surgically closing the esophageal-tracheal fistula. Children with this disability need careful care and proper nutrition.
tags: