This is an automatically translated article.
Article by Doctor Cardiology Interventional Unit, Vinmec Times City International General Hospital.Although mortality from coronary heart disease (BMV) has decreased significantly in many countries, CVD remains the leading cause of death among adults in developed countries and a leading cause of premature death. rapidly among adults in developing countries.
There is considerable interest in the diagnosis of CAD when the patient remains asymptomatic and before the development of hard endpoints (eg, myocardial infarction, sudden cardiac arrest), which is associated with increased incidence significant morbidity and mortality. However, questions still exist regarding the suitability and cost-effectiveness of BMV screening along with the optimal screening method.
This is largely due to a lack of evidence that screening for CVD can improve outcomes more than having a CVD risk assessment and taking appropriate primary precautions that target CMV risk factors known.
Issues surrounding BMV screening will be reviewed here, with particular emphasis on the effectiveness of available screening methods. Screening for CVD in patients with diabetes, generally the higher-risk population, will be discussed in detail separately.
1. Screening reason
Progressive obstructive coronary disease (BMV) may exist with minimal or no symptoms, with manifestations that may progress suddenly and/or rapidly.The first clinical presentation of CAD, acute myocardial infarction, unstable angina, or sudden cardiac death, is often associated with significant morbidity and/or mortality.
The rationale for early detection of CAD is that detection in the subclinical phase of the disease can allow reliable identification of subjects at risk for adverse cardiac events and appropriate therapy (eg, lowering lipids) may improve the prognosis of high-risk individuals.
Other reasons for screening include certain high-risk occupations (eg, pilots, bus drivers) where an acute cardiac event could endanger large numbers of people or those with at higher risk of developing CMV are starting an exercise program.
Although screening can identify patients with CMV at increased risk, there is little evidence that such screening actually improves outcomes.
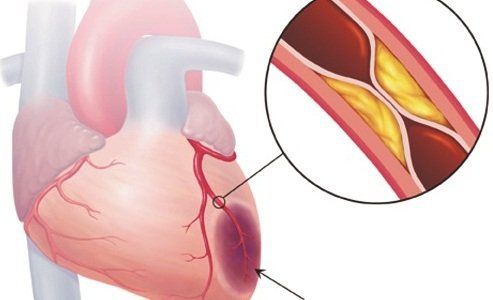
Bệnh mạch vành tắc nghẽn tiến triển (BMV) có thể tồn tại với tối thiểu hoặc không có triệu chứng
2. Purpose of Screening
The primary purpose of CAD screening is to identify patients whose prognosis could be improved by intervention (in this case, medical therapy for risk factors or coronary revascularization).Screening for CVD should be differentiated from an estimate of CVD risk (or overall CVD [CVD]). By definition, both are performed in asymptomatic individuals and both aim to improve outcomes with interventions, if indicated.
However, CVD (or CVD) screening identifies existing disease, while CVD (or CKD) risk estimates do not directly determine current disease but rather the likelihood of any future events related to CVD (or CKD).
Test results (screening or symptom-based) should be interpreted in the context of pre-existing disease likelihood (i.e. prior probability). The prior probability of CAD, over several decades, was based on patient age, sex, and features of angina symptoms and was confirmed using invasive coronary angiography.
Data obtained from computed tomography coronary angiography (MSCT scan) raise the possibility, however, that long established estimates of baseline frequency lead to an overestimation of risk. Additional data will be required to better define baseline frequency of BMV.

Mục đích chính của sàng lọc BMV là xác định bệnh nhân có tiên lượng có thể được cải thiện nhờ can thiệp
3. Consider Bayes
Understanding the theory of conditional probability (Bayes' theorem) as applied to medical decision-making is critical to understanding the utility of diagnostic testing for CAD in asymptomatic individuals.Knowledge of the baseline frequency of disease, along with the sensitivity and specificity of the tests performed, is necessary to determine the predictive value of the test performed. This is discussed in detail elsewhere.
The earliest likelihood of having CAD in a population has certain characteristics that influence the risk of CHD after infection. A positive result is likely to be a true positive (that is, a low false positive rate) in a population at high risk for CAD, while a negative test is likely to be a false negative.
In contrast, in a population at low risk for CMV, a positive test is only weakly correlated with the presence of BMV (i.e. has a high rate of false positives), whereas a negative test is more likely highly predictive of the absence of BMV. The results of the stress test (positive versus negative) had the greatest impact on differentiating the highest versus lowest probability of disease in the population from the pre-intermediate probability.
Therefore, the probability of post-test CMV is directly related to the specific population evaluated and the test results.
4. Access

Các câu hỏi nên tập trung vào việc phát hiện các triệu chứng đau thắt ngực
Trials in low-risk subjects may add to the cost of care without significant benefit, and active studies in low-risk patients are more likely to be false positives and have may lead to unnecessary tests and procedures.
In contrast, testing in asymptomatic individuals at high estimated CVD risk (who are already candidates for primary prevention with guided medical therapies) is unlikely to result in increased benefit, as negative studies in such high-risk patients are more likely to be false negatives.
History and physical examination — Most asymptomatic patients undergo routine maintenance checkups as part of routine care including focus history and physical examination; Along with this, it is necessary to estimate the short- and long-term CVD risks.
History and physical examination will rarely provide evidence of a diagnosis of CAD but will identify symptomatic patients requiring further evaluation for CAD.
● Personal history - Questions should focus on detecting symptoms of angina or angina as well as assessing lifestyle factors, including overall physical activity and fitness levels , dietary choices, smoking, alcohol consumption, illicit drug use, emotional stress, and sleep quality, all affect cardiovascular risk.
● Family history - A family history of early atherosclerotic disease or sudden cardiac death is often associated with an increased risk of CAD in screened patients.
● Calculation of risk scores - Although not providing a diagnosis of CAD, cardiovascular risk assessment is important to determine a primary prevention strategy. A variety of risk scores have been developed and validated in different populations, with no single risk score that is optimal for every patient. The approach to estimating cardiovascular risk in an asymptomatic patient is detailed separately.
5. Who should be screened?
The approach to screening for CVD is as follows:Screening does not apply to people with cardiovascular disease (CVD) or equivalent CVD risk; Such individuals are known to be at high risk for recurrent CKD events and should be treated with appropriate secondary precautions.
Screening does not apply to patients with symptoms suggestive of CAD, such as chest discomfort on exertion; Symptomatic individuals should be evaluated for CAD or other conditions with appropriate diagnostic testing as indicated.
Do not screen most asymptomatic adults for CAD. However, nearly all patients 20 years of age and older with no established CKD should undergo periodic cardiovascular risk assessment every 3-5 years. Select asymptomatic adult patients with 10-year or median increased CVD risk who may undergo coronary artery calcium (CAC) scoring to guide discussion of the risks of statin therapy.
BMV screening candidates are typically members of one or more "special populations" in which a BMV event may pose a unique or additional risk beyond those in the average population:
Advocacy athletes prior to participation People with high-risk occupations or hobbies People with occupations related to public safety or the lives of others CMV screening in asymptomatic patients with diabetes , generally a population at higher risk of cardiovascular disease, will be discussed separately.

Bệnh nhân bị đái tháo đường sẽ không được thực hiện sàng lọc bệnh mạch vành
6. Special populations
Pre-Participation Trial — Pre-participation assessment of asymptomatic patients varies slightly depending on whether the athlete's goal is recreational or competitive:6.1 Performer For those In asymptomatic patients who are fairly sedentary and plan to begin a recreational exercise program, no pre-participation testing is required prior to initiating an exercise program. However, some patients may require reassurance that they will be able to actively exercise; in such cases, medical authorization is recommended, with exercise testing at the discretion of the provider according to the American College of Sports Medicine.
As an example of the utility of stress ECG testing before starting an exercise program, only 2% of the 3617 asymptomatic, hypercholesterolemic men underwent ECG testing at initially experienced an acute activity-related cardiac event during follow-up (median 7.4 years).
Despite a 2.6-fold increased risk of cardiac events in clinically silent patients, exercise-induced ST-segment changes in the suboptimal treadmill trial (ETT) of study participation In the study, only 11 of 62 men who experienced an activity-related event had a positive ETT on entry (sensitivity 18%).
6.2 Competitive Athletes Professional associations in both North America and Europe have published recommendations for pre-participation screening for young competitive athletes (those under the age of 35). A full discussion of pre-screening for competitive athletics is presented separately.
Public safety occupations, high-risk occupations, and high-risk recreational activities — Some asymptomatic patients have occupations related to public safety (eg, airline pilots, drivers). bus, truck driver) or a high-risk occupation or hobby (e.g., diver) that is required by regulatory or regulatory agencies for routine check-ups as part of a routine health assessment .
In such patients, specialists usually conduct the required testing. In the absence of any required testing, specialists do not perform routine screening or pre-participation testing in these asymptomatic patients.
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical professionals, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space. Customers when choosing to perform tests here can be completely assured of the accuracy of test results.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.