This is an automatically translated article.
Posted by Specialist Doctor II Phan Phi Tuan - Department of General Surgery - Vinmec Phu Quoc International General HospitalSituations of victims with respiratory burns are often caused by fire, especially in closed rooms, closed vehicles...; burns from explosions caused by explosions in mines, explosions of soup-de pots with steam under high pressure. In addition, there may be cases of respiratory burns due to hot liquids, liquid chemicals causing burns to the airways when the head is submerged like falling into a hot lime pit. .
1. Overview of respiratory burns
1.1 Causes and causative agents of respiratory burns Respiratory burns are caused by inhalation of burning agents such as fire, hot gas, hot steam, exhaust gas from automobile engines, motorbikes, generators, gas, etc. Coal smoke, half-burnt firewood or chemical products formed from combustible cause damage to the respiratory organs. In addition, there may be cases of respiratory burns due to hot liquids, liquid chemicals causing burns to the airways when the head is submerged like falling into a hot lime pit..Circumstances of the victim being burned The respiratory tract is often caused by fire, especially in closed rooms, closed vehicles...; burns from explosions caused by explosions in mines, explosions of soup-de pots with steam under high pressure. The longer the victim is exposed to the heat source, the more severe the burn. Mortality rate is high, especially in 24-48 hours after respiratory burn, death can be over 50%.
1.2 Pathogenesis of respiratory burns Experimental research on causing respiratory burns by flame sprayed into the cat's mouth shows that: Burned parts in descending order are pharynx, pharynx, larynx, trachea, bronchi. and alveoli. The temperature of the causative agent decreases gradually as it goes deeper into the respiratory system (the temperature in the mouth is 3500C -5000C, the temperature in the larynx will be from 1500C-350oC; in the upper part of the trachea up to from 3500C - 5000C). 800C-1000C only about 650C–950C remaining in the trachea).
The blood temperature in the left ventricle of the heart is also up to 44oC; while the circulating blood temperature in the pulmonary parenchymal meshwork may be hotter. Blood in the superior vena cava has a higher temperature rise than in the superior aorta. In experimental studies, respiratory burns always lead to edema and congestion of the respiratory mucosa. The permeability of the pulmonary capillary wall is increased due to the heating of the blood flow in the capillaries, leading to the escape of plasma fluid in the lung parenchyma. The blood circulation in the small circulation is stagnant due to high pulmonary artery blood pressure, in addition, there are many venous thromboembolisms in the lung parenchyma. The edematous fluid that escapes through the microvascular wall of the lung parenchyma contains up to 80% albumin, which accumulates in the interstitial space and will be hyalinized, causing progressive respiratory depression.
Clinically, there is a phenomenon of airway obstruction by secretions of sputum, the plugs caused by the hematopoietic clumps, the necrotic mucosal cells and leukocytes form the obstructions of air circulation. . Swelling in the face and neck due to burns and burns in the chest will interfere with the cough reflex to expel the sputum. The cough reflex is also lost when there is necrosis of the respiratory mucosa and nerve endings are damaged.
The above phenomena lead to emphysema, collapsed lung segments due to obstruction. There is an inflammation of the original trachea spreading to the small bronchi, surrounding tissues around the bronchi and then to the lung parenchyma. In patients with respiratory burns, there is often a decrease in maximal ventilation, lung vital capacity, oxygen utilization index, and oxygen pressure in the blood.
Presence of acidosis with elevated prostacyclin concentrations in the lymphatic system of the lungs. Thus, in the time of respiratory burn and smoke inhalation injury, acute respiratory failure, followed by pulmonary edema from 48 to 72 hours after the burn, and complications of bronchitis from day 5. to the 7th day after the burn.
The pathological role of PAF (Platelet activating factor), thrombosanne A2, free oxygen radicals.... has also been studied in respiratory burns. According to a previous study that recorded 97 fire burn victims in 4 passenger cars, 60% had combined respiratory burns. Monitoring clinical progress in 55% of respiratory burn victims found that there were 1.7% cases of acute respiratory failure with alveolar hemorrhage; 27.5% pneumonia and 8.6% bronchitis.

Hình ảnh bệnh nhân bỏng hô hấp nặng
2. Diagnosis of respiratory burns
2.1 Epidemiological factors Victims suffer burns in an enclosed space such as fire in a closed room, inhalation of hot steam in a closed bathroom, underground fire, patient self-immolation .......With children, it is necessary to concern about respiratory burns for children who choke, inhale hot liquid from the airways by falling face down on the burn agent. Burns to the head, face, neck and chest with burns to the lips. Hot liquids or chemicals seep into the lining of the nose, mouth, and throat. Breathing in a lot of smoke and combustion products.
2.2 Clinical manifestations Difficulty swallowing, discomfort in the throat Difficulty speaking or loss of voice due to swelling of the vocal cords Dry cough, then cough with thick soot-colored sputum, possibly foamy cough with blood jets. Burned nose hairs Swollen tongue When examining the nose and throat, you can see: The mucous membranes of the mouth, nose, pharynx, and larynx are congested, red, on a congested background with grayish white fibrin membranes, edematous tongue, laryngopharyngeal edema and edema of the larynx. vocal cords. Deep burns may show white necrotic patches on the mucosa. Increased secretion of phlegm and drool in the respiratory tract. Respiratory distress syndrome due to edema of the glottis, tracheobronchial mucosa, gradually increasing dyspnea, shallow tachypnea, decreased bronchioles, rales, rales, excitability, and malaise. May be accompanied by explosion wave syndrome, CO poisoning, CO2, poisoning by products in smoke, chemicals.
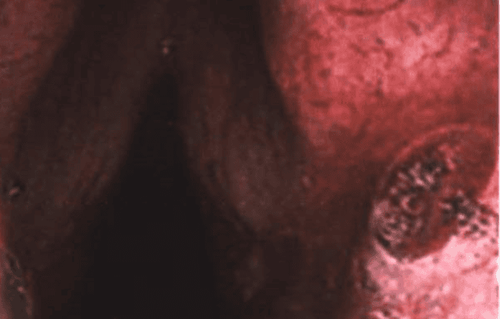
Viêm loét ngay khe thanh môn trên nền phù nề sung huyết mạnh do bỏng hô hấp.
Performing other tests also noted some variation. Arterial blood PO2 can be reduced to 75 mmHg, the deeper the burn injury, the more severe the arterial hypoxia, can be below 50 mmHg. The normal lung capacity of 3,500 - 5,000ml can be reduced, in some cases it can be reduced to 80-1,300ml. PaO2/FO2 below 400 indicates a pathological disorder, if less than 200 indicates severe respiratory failure, requiring assisted respiration using positive end expiratory pressure (PEEP) to prevention and treatment of alveolar collapse. PaCO2 can be as high as 50mmHg.
Breast volume expansion is reduced by up to 50%. At the same time, there is anemia due to the destruction of red blood cells, if the respiratory burn is accompanied by skin burns with a total burn area of about 21% - 50% of the body area, the volume of red blood cells can be destroyed up to 15%, if the total burn area is more than 50% of the body area, the red blood cell volume is destroyed up to 29%, if only the skin burns due to heat alone, the red blood cell volume is only destroyed about 14%. The blood is concentrated due to the increased permeability of the pulmonary parenchyma microvasculature to drain more plasma into the interstitial space with a hematocrit of about 60% - 72%. The viscosity of blood increases as high as 6.9 - 8.2. Urea, blood creatinine increased. The circulating blood volume is much lower than in simple burns with the same burn area, the arterial blood pH shifts towards respiratory acidosis.
3. Classification of respiratory burns
Mild burns: Normal voice, mild respiratory disorder, oropharyngeal discomfort, no cyanosis, few pneumonia complications or if present, the course is not severe, chest X-ray is normal.Moderate burn: Hoarse voice, severe respiratory distress, cyanosis, rough breathing sounds, rales rales, rales snoring; often have pneumonia complications with quite severe course; respiratory failure and heart failure grade I, II.
Severe burns: Severe hoarse voice, severe shortness of breath, possible shortness of breath, cyanosis, distended neck veins, hoarse cough or thick sputum, respiratory failure and severe acute heart failure; emphysema, atelectasis of lung segments, necrosis. In the final stage, acute pulmonary edema is common, which can easily lead to death. Usually death is most common in the first days after burns; and death due to complications of pneumonia, due to complications of systemic infection usually after 3-20 days.
4. Treatment of respiratory burns

Tại cơ sở y tế, bệnh nhân sẽ được cho sử dụng thuốc giãn phế quản, chống viêm
Quickly remove the victim from the smoke and heat, make sure the victim is in a safe, well-ventilated place. Extinguish a burning fire by covering yourself with blankets or rolling on the ground, pouring water, and removing burning clothing. For emergency people, when entering a closed pgong1, it is necessary to have careful protective equipment. If the victim is conscious, make sure the victim's airway is open; Remove the foreign body in the oral cavity (if any). If the victim vomits, place the victim on his side to prevent vomiting, back inside, causing respiratory obstruction. If the victim stops breathing, give artificial respiration and squeeze the heart out of the chest. Soak in clean water to clean the burned body part, apply light pressure, and give oral rehydration. Go to the nearest medical facility. First aid at the facility:
Remove all foreign bodies, secretions (if any) in the nasal cavity and airways Perform artificial respiration if indicated. Leave the patient to lie motionless and quiet. For the patient breathe 100% oxygen if CO poisoning Cardiovascular support, respiratory aid Nebulizer, bronchodilator, anti-inflammatory, reduce edema Give sedatives, relieve pain Practice breathing, cough and expectorate to avoid congestion of phlegm Open air emergency management when severe respiratory failure, other methods are not effective Prevention and treatment of shock Quickly transfer the patient to a specialized hospital Specialized line:
Conduct endoscopy to diagnose respiratory burns and treat treatment of inflammatory complications, acute respiratory failure (intubation, tracheostomy, assisted ventilation), sputum aspiration, aerosolization, breathing exercises... Vinmec International General Hospital with system With a system of modern medical facilities, equipment and a team of experts and doctors with many years of experience in medical examination and treatment, patients can rest assured that they will be examined and treated at the Hospital.
To register for examination and treatment at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register online HERE.
MORE:
Correct first aid for potty burns, thermal burns First aid for fire burns, boiling water burns Grades of burns