This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
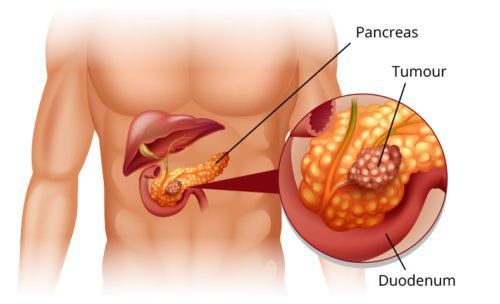
Pancreatic carcinoma (PDAC) carries significant morbidity and mortality and remains one of the most difficult malignancies to treat. Individual patient and tumor factors need to be taken into account to provide an optimal, personalized approach. In this review, we highlight established and novel biomarkers that have the potential to be used as prognostic biomarkers in pancreatic carcinoma and some of which may be used to guide treatment decisions.
1. Pancreatic Carcinoma Overview
Despite great advances in the treatment of many solid tumors, survival rates in pancreatic carcinoma have not improved. Delayed diagnosis, aggressive biologics, and marked chemoresistance all contribute to this disappointing trend. Prognostic biomarkers inform the likelihood of cancer occurring (recurrence, progression, or death) independent of the type of treatment.
A biomarker is predictive if there is a difference in treatment efficacy in biomarker-positive versus biomarker-negative patients. General prognostic markers, which are not specific to a defined treatment regimen, may be useful in distinguishing which patients are at high risk for a poor outcome and therefore require more aggressive management. While large gene expression panels have been identified for use in the prognosis of other malignancies and some are associated with treatment response, several such markers have been well characterized in cancer. pancreatic cancer and even less are used in clinical practice.
Các tiến bộ y học chưa đem lại hiệu quả cao trong việc điều trị ung thư biểu mô tuyến tụy
2. Serum-based biomarkers (blood tests)
There are few clinically used biomarkers for pancreatic adenocarcinoma compared with other malignancies. Carbohydrate antigen 19-9 (CA 19-9), or sialyl Lewis antigen, is the only biomarker recommended by the National Comprehensive Cancer Network guidelines for the evaluation of carcinoma. pancreas . Its role in carcinogenesis may be related to its association with increased adhesion of cancer cells to endothelial cells through E-selectin. In addition to its well-known role in the diagnosis of pancreatic adenocarcinoma, higher preoperative CA levels have been shown to correlate with advanced stage, less likelihood of resumption, and reduced survival. omission. However, its sensitivity is limited because 10% of the population is non-CA 19-9 secretagogue and its specificity is limited because it is secreted by the normal biliary epithelium.
Other commonly used preoperative markers include carcinoembryonic antigen (CEA), intercellular adhesion glycoprotein usually present at very low levels in the blood, and lactate dehydrogenase (LDH), an enzyme involved metabolize sugar and C-reactive protein (CRP), an acute phase reactant. Compared with normal levels, elevated LDH, CEA, and CRP have all been shown to be independent prognostic factors for adverse survival. However, similar to CA 19-9, these laboratory markers are limited in specificity.

Kháng nguyên carbohydrate 19-9 giúp chẩn đoán ung thư biểu mô tuyến tụy
3. Growing Blood or Serum-Based Biomarkers
The value of serum-based markers is their less invasive approach and ability to collect multiple samples for different analyses. The most notable serum-based markers currently being investigated include circulating tumor cells, circulating tumor DNA, and microRNAs.
Metastasis is often considered one of the newest steps in cancer progression; however, the presence of circulating tumor cells (CDC) in the early stages as well as in pre-invasive lesions has challenged this. Circulating tumor cells are cancer cells that have been shed from the primary or metastatic tumor and can travel through the bloodstream, potentially leading to new metastases.
4. Histology-based biomarkers
High-quality pancreatic tumor biopsies
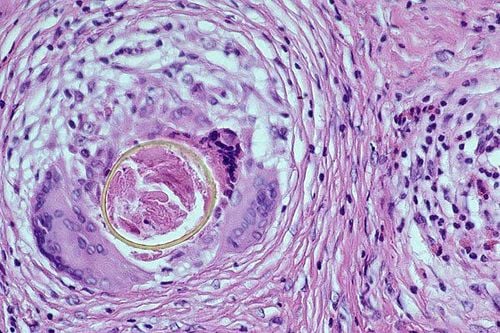
There have recently been significant advances in the ability to obtain histologically intact core biopsies from pancreatic cancer, and this change will likely allow for a wide range of uses. than tissue-based biomarkers. Although few studies have evaluated different biopsy techniques and needle designs side-by-side, it is clear that the newer generation of "core" microneedle (FNB) biopsies will provide excellent specimens. much better quality and quantity than first-generation fine-needle biopsies (FNA).
Several studies have demonstrated that the overall diagnostic accuracy of FNA and FNB is comparable (92.5- 94.8% vs 90-98.3, respectively). In some studies, FNB required a significantly lower number of needle passes and was associated with higher accuracy in situ cytology. However, more recent studies have found similar overall diagnostic accuracy and pathological accuracy.
Lấy mẫu mô tuỵ để chẩn đoán qua kỹ thuật siêu âm nội soi
5. Prognostic markers
Tissue-based markers offer the benefit of being more specific to tumor tissue, but at the expense of requiring more invasive collection techniques. Immunohistochemical analysis (IHC) is a widely used procedure used to visualize specific molecular markers and determine their distribution in clinical tissue samples.
Although these markers may be useful in patients undergoing surgical resection, investigation is still needed to determine if there is prognostic value for these biomarkers in brush or biomarker samples. preoperative or not.
SPARC factor
Acidic and cysteine-rich secreted protein (SPARC) is a stem cell glycoprotein that undergoes epigenetic silencing in pancreatic adenocarcinoma, but is often expressed strongly at the faecal surface space between tumor and stroma by stromal fibroblasts. Supportive data suggest that this interaction is important for tumor progression, metastasis, and chemotaxis.
SPARC stromal expression was observed in all disease stages suggesting that early expression is critical for tumor progression. Strong stromal SPARC expression in well-to-moderately differentiated cancer patients who underwent surgical resection was associated with reduced survival compared with patients without SPARC expression. Furthermore, patients with diffuse stromal SPARC expression beyond the periabdominal region have a significantly worse prognosis.
Smad4 factor
Smad4 is a tumor suppressor gene involved in transforming growth factor beta (TGF-B). As evidenced by its alternative name, DPC4 (deleted in pancreatic carcinoma, site 4), loss or inactivation of Smad4 is seen in ∼50% of pancreatic carcinomas and results in increased cell proliferation. cells by regulating progression from G1-S in the cell cycle. Loss of Smad4 expression has often been shown to be associated with reduced survival in pancreatic carcinoma.
Interestingly, one study contrastedly demonstrated that low Smad4 expression is associated with improved overall survival and, importantly, pancreatic resection only (through time) benefit. live longer) tumors that have lost Smad4 expression.
KRAS factor
KRAS (V-Ki-ras2 Kirsten mouse sarcoma oncogene) is a GTPase that activates proteins required for the transmission of growth factors and other cell signaling receptors. Overall, KRAS mutations were correlated with reduced survival. The different mutant subtypes showed different survival times, with wild type GGT (glycine) converted to GAT (aspartate) being the most common and the only one that was predictive of viability poor omission.
In addition, mutation analysis performed for these KRAS mutations can be performed by quantitative polymerase chain reaction (PCR), which is cheaper and faster than other sequencing methods and uses less data. more DNA data, making it easier to perform multiple molecular analyzes on the same sample.
Smad4, hENT1 and SPARC have another benefit as biomarkers, in that they have been shown to be effective on preoperative biopsies. As quantitative PCR of VEGF and KRAS has also been shown to be accurate, there may be a role for these biomarkers during preoperative evaluation with biopsy-related smaller samples.
6. Biomarkers predict treatment
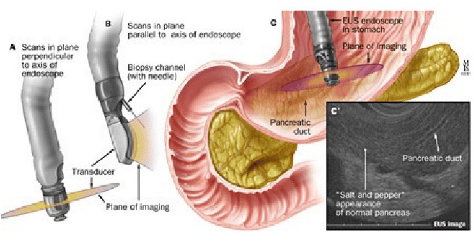
There are different imaging modalities involved in the diagnosis and staging of pancreatic carcinoma including computed tomography (CT), magnetic resonance imaging (MRI), endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP). The role of these modalities has changed over time, but the relative importance of EUS has increased dramatically with the introduction of EUS-guided needle aspiration (EUS-FNA) over 20 years. prior to. Although limited by relative invasiveness and operator variability, it has been shown to have excellent sensitivity (91-100%) and specificity (94-100%) for diagnosis. pancreatic carcinoma.

Chụp CT có vai trò cho phép hẩn đoán ung thư biểu bì tuyến tụy
7. Role of VEGF inhibitors, Vatalinib and nab-paclitaxel
In addition, from many other cancer treatment algorithms, the authors know that it is important to understand changes in tumor biology following the first treatment regimen. Recent phase II trials of the VEGF inhibitor, Vatalinib, and nab-paclitaxel as separate second-line therapy in advanced pancreatic carcinoma demonstrated a favorable survival outcome in some patients; however, serum-based biomarkers were not correlated with response and the predictive value of tissue-based biomarkers (SPARCs) was inconclusive due to the small sample size. With high-quality biopsies, we can expect that most trials, and increasingly standard practice, will emphasize the need for post-treatment biopsies.
CONCLUSION
The most promising tissue biomarkers include hENT1, SPARC, Smad4 and VEGF as they may be of value in the preoperative period and may also have predictive value in guiding management individual pancreatic cancer treatment. The novel serum-based markers are also valuable due to their minimally invasive approach and are fundamental for genetic analysis. As both endoscopic approaches to obtaining high-quality biopsies and the molecular understanding of pancreatic cancer advance, it is likely that these and many other biomarkers will be included. routine clinical practice.
Vinmec Hospital with modern facilities and equipment and a team of experienced professionals, always dedicated to medical examination and treatment, customers can be assured of gastroscopy and esophagogastroduodenoscopy services. at Vinmec International General Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
ReferencesYadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144(6):1252-1261. Swords DS, Firpo MA, Scaife CL, Mulvihill SJ. Biomarkers in pancreatic adenocarcinoma: current perspectives. Onco Targets Ther. 2016;9:7459-7467. Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, Fernandez-delCastillo C, Warshaw AL. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J Clin Oncol. 2006;24(18):2897-2902.