This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
Patient has a persistent cough, goes to many doctors, but still no relief. It was time to see a gastroenterologist, found that the patient had reflux esophagitis, and the doctor concluded that the patient's cough was caused by reflux esophagitis. What are the characteristics of this disease? Why can reflux esophagitis cause a persistent cough? This article will cover that issue
1. Chronic cough (also called persistent cough)
Cough is defined as chronic when it lasts more than 8 weeks; A much more persistent cough is defined as a chronic cough that is intractable. Common causes of chronic cough are side effects from commonly used medications (especially ACE inhibitors), tracheomalacia, chronic obstructive pulmonary disease (COPD), bronchiectasis. , asthma, obstructive sleep apnea, meningitis, and gastroesophageal reflux disease. In non-smoking, normal chest X-rays without ACE inhibitors, chronic cough was identified in 86% of cases as asthma, postnasal drip syndrome (PNDS), and Gastroesophageal reflux disease, although often multiple causes coexist.
2. The relationship between chronic cough and gastroesophageal reflux disease
Several studies show a significant association between chronic cough and gastroesophageal reflux disease, with prevalence ranging from 10% to 56%, mainly due to physician referrals from other specialists to specialized centers. In a large prospective European study, the PRO study of gastroesophageal reflux disease, chronic cough could be attributed to gastroesophageal reflux disease in 13% of patients. core. In a recent systematic review, Irwin et al identified gastroesophageal reflux disease as the cause of 85% of chronic coughs worldwide, especially in Western countries. In Japan, gastroesophageal reflux disease was described as a rare cause of chronic cough, accounting for only 7.7% of all causes. Lower obesity rates and less common Western diets are the main factors associated with the rarity of gastroesophageal reflux disease in this country.
Gastrointestinal symptoms may be absent when GERD causes a cough
When GERD causes a cough, digestive symptoms may be absent up to 75% of the time, making diagnosis more difficult. Furthermore, cough and gastroesophageal reflux disease are common and often coexisting diseases, but an association does not imply a causal relationship in all cases: Eastburn et al. flags in 25% of cases. The time relationship between reflux episodes and cough may help accurately resolve chronic cough with reflux, although diagnostic gold standards are lacking.
Triệu chứng ho có thể do bệnh trào ngược dạ dày thực quản gây ra
Pathogenesis of gastroesophageal reflux cough
Two main theories proposed to explain the cough associated with gastroesophageal reflux disease are the reflex theory, which considers cough to be a consequence of reflexes The vagus-mediated esophagitis caused by reflux and regurgitation theory, suggests that a regurgitated aspiration behavior in the trachea is the cause of the cough.
3. Diagnosis of cough due to gastroesophageal reflux disease
Cough due to gastroesophageal reflux disease is usually a dry cough and is often aggravated by changes in posture, food intake, and pronunciation. Chronic cough is often the only manifestation of gastroesophageal reflux disease. In patients presenting with a chronic cough, lung disease should first be ruled out by performing a radiological examination, such as a chest x-ray or computed tomography (CT) of the lungs. Some cases require bronchoscopy for diagnostic or therapeutic reasons.
Laryngoscopy signs
When gastroesophageal reflux disease causes cough due to irritation of the larynx, laryngoscopy may demonstrate signs consistent with "reflux laryngitis". During bronchoscopy, abnormalities consistent with aspiration can be detected, such as sublaryngeal stenosis, tracheobronchial hemorrhage, and congestion of the accessory bronchi. Evidence of inflammation and edema of the larynx and lower airways should not automatically translate to gastroesophageal reflux disease as these findings may be related to other causes of cough or to the cough itself. . If imaging and endoscopy are normal, it can be assumed that gastroesophageal reflux disease causes cough by stimulating the esophageal-bronchial reflex. In GERD, there are many potential cough mediators other than acid, so several possible mechanisms are suggested.
Gastroesophageal endoscopic signs
Patients with laryngeal or pulmonary manifestations of gastroesophageal reflux disease are usually examined first by an otolaryngologist, and only if they have symptoms. Only the second time, they are admitted by a gastroenterologist. In such typical situations, an upper gastrointestinal endoscopy is often indicated.
Normal esophagoscopy ( esophagogastroduodenoscopy ) is a common finding in patients with cough due to gastroesophageal reflux disease ; Only a few have esophagitis or Barrett's epithelium. Therefore, a normal esophagogastroduodenoscopy does not rule out the presence of gastroesophageal reflux disease or associated pulmonary abnormalities. Therefore, upper endoscopy should not be performed to diagnose asthma, chronic cough, or laryngitis associated with gastroesophageal reflux disease. Furthermore, the diagnosis of esophagitis did not confirm a relationship between gastroesophageal reflux disease and potential extraesophageal manifestations.
Role of 24-hour esophageal pH monitoring
While 24-hour esophageal pH monitoring can only detect acid reflux episodes, impedance-pH monitoring can also detect non-acid reflux. During impedance-pH monitoring, reflux episodes are detected when characteristic impedance changes (eg, progressive change in intraoral impedance) are considered, while pH data are used. used to distinguish acid from non-acid reflux. A temporal association between reflux events was detected on 24-hour reflux monitoring and symptoms were determined by symptom index (SI) and symptom association probability (SAP).
Esophageal manometry and pH monitoring in addition to PPIs may be recommended in patients with cough unresponsive to treatment and who are considered surgical options.
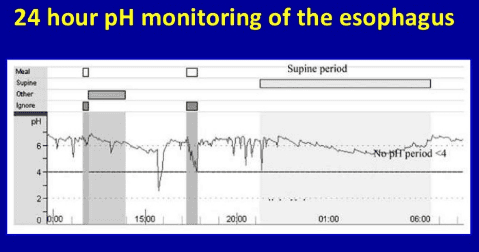
Một kết quản của đo pH thực quản 24 giờ
Recently, Burton et al proposed to use scintigraphy with Tc-99m to identify changes in esophageal motility and pulmonary aspiration of refluxed material.
Because of its low pH monitoring capabilities, its invasiveness, and the common association between chronic cough and gastroesophageal reflux disease, it is common to diagnose a cough associated with gastroesophageal reflux disease by empirical PPI testing. Up to 79% of patients with cough secondary to GERD resolved symptoms after PPI treatment, thus confirming the diagnosis. However, the American Gastroenterological Association (AGA) Guidelines recommend 24-hour pH monitoring prior to initiating PPI trials in patients suspected of having extraesophageal manifestations associated with gastroesophageal reflux disease. management and no typical esophageal findings.
4. Treatment of cough caused by reflux esophagitis
Although there is little evidence to support this approach, PPIs are the most common treatment used in cases of suspected chronic cough due to gastroesophageal reflux disease. Several studies have shown improvement of chronic cough with this treatment; however, a recent randomized controlled trial (RCT) did not show a difference between PPIs and placebo. Explanation can be found in the small sample size included and in the types of quality of life (QoL) questionnaires used to address the usefulness of treatments.
A Cochrane systematic review reported insufficient evidence to conclude on the efficacy of PPIs in the treatment of cough associated with gastroesophageal reflux disease, although some beneficial effects were seen in one study. sub analysis. Chronic cough has a high response rate to placebo, and this fact hinders statistical results in clinical studies. Clinicians prescribing PPIs should consider their potential side effects, and maintenance treatment should be planned only when proven helpful.
Role of PPI antisecretory drugs
Chang et al., in a meta-analysis of RCTs comparing PPIs with placebo, demonstrated therapeutic efficacy in patients with cough associated with gastroesophageal reflux disease. esophagus in a subgroup analysis. In the meta-analysis, there was no effect on primary outcomes, although all studies supported PPIs. The number needed to treat (NNT) for an effective cough treatment was 5. The authors demonstrated a smaller cough treatment effect compared with the results of the uncontrolled trials, probably related to the effect. placebo, as high as 85%. A limitation of this meta-analysis is the lack of data from RCTs including patients with chronic cough without gastroesophageal reflux disease. Furthermore, in the included studies, there were no consistent data on the effectiveness of dietary changes or surgical treatment.
In 2006, the American College of Chest Medicine (ACCP) Guidelines on Cough Reflux Syndrome were published. These guidelines recommend behavioral changes such as weight loss in overweight patients, elevating head to bed, and avoiding eating three hours before bedtime. PPI therapy is recommended in patients with symptoms of heartburn and regurgitation; In people with cough but no gastric symptoms, PPIs alone should not be indicated, although they may be considered in combination with lifestyle modifications. In the latter case, prescribing PPIs without changing behavior is unlikely to resolve symptoms.
While gastrointestinal symptoms usually resolve after 4-8 weeks of treatment, the literature shows that improvement in cough can take up to 3 months. In general, a positive response to PPIs is evident within a few weeks, which is the strongest indicator of disease resolution. It is important to reassess the patient's response early to avoid prolonged use of futile therapies.
Some experts recommend an initial twice-daily dosing of PPIs in patients with chronic cough, although some studies show no superiority of twice-daily regimens over once-daily regimens. day. In resistant cases, the addition of a histamine H2 receptor antagonist (H2 blocker) and/or baclofen may be helpful.

Điều trị nội khoa được sử dụng trong trào ngược dạ dày thực quản
Anti-reflux surgery (such as Niessen's fundraising method) may have a role in refractory chronic cough in the absence of a major motility disorder (no bowel movements, increased tone, distal esophageal spasm, increased contractility).
Vinmec International General Hospital examines and treats gastroesophageal reflux disease with the most optimal internal - surgical methods for patients, both children and adults. Coming to Vinmec International General Hospital, patients will receive direct, dedicated and professional examination from a team of qualified and experienced medical staff.
If you have a need for consultation and examination at Vinmec Hospitals under the national health system, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
ReferencesMarilena Durazzo,1,2,* Giulia Lupi, Extra-Esophageal Presentation of Gastroesophageal Reflux Disease: 2020 Update, J Clin Med. 2020 Aug; 9(8): 2559 Vakil N., Van Zanten S.V., Kahrilas P., Dent J., Jones R., Global Consensus Group The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus. Am. J. Gastroenterol. 2006;101:1900-1920. doi: 10.1111/j.1572-0241.2006.00630.x. [PubMed] [CrossRef] [Google Scholar]