This is an automatically translated article.
Pleural effusion is the accumulation of too much fluid in the lungs or between the lungs and the ribcage, putting pressure on the lungs making it difficult for the patient to breathe. One of the effective solutions to treat pleural effusion is thoracoscopic surgery causing adhesions to the pleura.
1. What is pleural adhesion?
Pleural adhesion is a method of causing adhesion of the parietal leaves to the visceral leaves of the pleural cavity with the aim of avoiding the accumulation of fluid or gas in the pleural space, preventing the risk of pleural effusion. .
Common pleural adhesion methods:
Through pleural drainage Thoracoscopy (under local anesthesia and anaesthesia) Open thoracoscopic surgery to adhere pleura
2. Open chest surgery to create pleural adhesions
Thoracotomy with pleural adhesions is minimally invasive surgery with small incisions (less than 8cm)
2.1 Indications Cases in which pleural effusions are due to malignant causes, causing rapid recurrence of fluid (>500ml) / 24 hours). Permeable pleural effusions recur rapidly and other treatments are ineffective. Pneumothorax recurs many times, in patients with pulmonary fibrosis, many air cysts are scattered throughout the lung that cannot be treated completely by surgery.
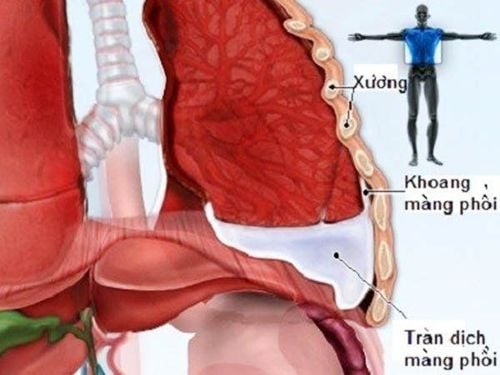
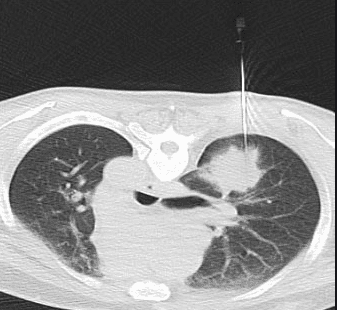
Tràn dịch màng phổi cần được chỉ định phẫu thuật mở ngực tạo dính màng phổi
Patients with damaged contralateral lung, unable to conduct ventilation of one lung or pleural space Adhesions make thoracotomy difficult. People with serious systemic diseases such as: unstable hemodynamic status after trauma, blood diseases, severe chronic diseases, previous chest trauma... Patients with hyperthyroidism have contraindications to Povidine iodine. Patients with severe coagulopathy cannot have a pleural drain. The pleural space is heavily walled.
2.3 Preparation for preoperative thoracotomy to create pleural adhesions The composition of the operating team is a total of 7-8 people including:
Surgical team: 1 surgeon, 2 surgical assistants, 1 nurse serving surgical instruments , 1 run outside the specialty. Specialist anesthesia team: Anesthesiologist and 2 assistants
2.4 Preoperative preparation for the patient Before conducting thoracotomy with pleural adhesions, the patient is carefully examined clinically, cleaned, prophylactic antibiotics, anesthetized and resuscitated. Patients and families are explained and guided about the surgical procedure as prescribed, and legal documents are completed.
Surgical instruments : Major surgery kit for conventional thoracotomy (preparation).. Equipment to assist in opening and closing the thorax (ribs, rib only...) or opening and closing. sternum. Anesthesia equipment: Anesthesia kit for thoracic surgery, anesthetic and cardiovascular resuscitation drugs, double-bore endotracheal tube (Carlens)...

Phòng mổ và dụng cụ cần được chuẩn bị đầy đủ trước khi tiến hành phẫu thuật
3. Surgical procedure to treat chest wound infection
3.1 Patient position At the beginning of surgery, the patient is placed in a 90-degree lateral position to the opposite side depending on the site of the surgical wound infection on the chest wall.
3.2 Endotracheal Anesthesia The anesthesiologist conducts double-lumen endotracheal anesthesia.
3.3 Procedures Make an incision less than 8cm in the small thorax anterior, lateral, or lateral through the V intercostal space between the anterior and medial axillary lines into the pleural space (this incision is usually non-muscular, use an adequate costal ball). . Into the pleural space, pair of endotracheal tubes on one side, to cause atelectasis on the injured side. Identify the lesion and evaluate the total lesion of the area in relation to other components in the thoracic cavity. Prepare patient: 2 barrel; Monitor electrocardiogram and capillary oxygen saturation (SpO2) continuously. Place two central and peripheral intravenous lines. Place patient on mechanical ventilation with 100% oxygen support and catheterization.
Burn or suture the air cysts (if any) in the lung parenchyma. Spray a mixture of talcum powder or Betadine on the surface of the lung parenchyma and the inner surface of the chest wall. In some cases, small gauze can be used to gently rub the surface of the chest wall (leaf parietal pleural cavity) to induce pleural adhesions. Check for bleeding and place a pleural drain. Lung expansion. Close the small opening and end the surgery.

Bệnh nhân được đặt dẫn lưu khoang màng phổi
4. Monitoring and identifying complications after surgery
4.1 Post-operative follow-up Monitoring and evaluating the overall condition: Pulse, blood pressure, temperature, drainage system... Give the patient antibiotics for intravenous infections, pain relief, blood transfusion and blood replacement solutions... depending on hemodynamic status and test results. Perform respiratory therapy from the first day after surgery. Indications to withdraw drainage when:Clinical: No air drainage and fluid index <100ml/ 24 hours X-ray image shows good lung expansion. Adjuvant adhesions through drainage can sometimes be caused if thoracoscopic adhesions fail.
4.2 Common complications Common adverse events associated with adhesion agents:
Chest pain Fever Infections of the pleural cavity Tachycardia Tachycardia pleural effusion Respiratory failure Common complications related to the surgical method :
Bleeding pleural : due to blood from the blood vessels of the chest wall, mediastinum or lung parenchyma are damaged overflowing into the pleural space.

Bệnh nhân có thể xuất hiện tình trạng sốt cao sau phẫu thuật
Subcutaneous pneumothorax: during surgery, the broken ribs punctured the spleen, causing pleural tears and parenchyma. Difficulty from the lung will escape through the pleural cavity and then through the parietal leaf tear to overflow into the chest wall organization under the skin, causing deformation and swelling. Atelectasis: This complication can occur when the patient is not breathing well and has blocked sputum after surgery. Recognizing signs are that the patient has difficulty breathing, fever, alveolar murmurs, X-ray images show atelectasis. To handle it, it is necessary to help the patient relieve pain, use systemic antibiotics, help the patient sit up and shake, cough and sputum, bronchoscopy (if necessary).
Open thoracotomy to create pleural adhesions is a widely indicated method for unfortunate patients with repeated pleural effusions. Patients should also follow all of their doctor's instructions during surgery and treatment to improve their chances of cure and reduce the risk of complications.
To register for examination and treatment at Vinmec International General Hospital, you can contact the nationwide Vinmec Health System Hotline, or register online HERE.