This is an automatically translated article.
Occipital gynaecomastia is a congenital malformation, characterized by abnormalities of the brain in the occipital cervical position. This type of malformation is usually treated with surgery. The goal of occipital hinge deformity surgery is to alleviate symptoms of the disease or prevent progression of spinal cord hollowness.
1. Overview of the occipital hinge deformity
1.1 What is occipital hinge deformity?
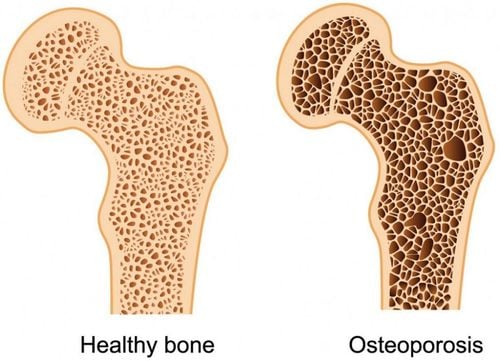
Occipital hinge deformity also known as occipital neck malformation, Chiari malformation is considered a rare birth defect (incidence less than 0.1%). This is a condition in which brain abnormalities occur in the occipital position, characterized by a low migration of the cerebellar amygdala through the occipital foramen. Most cases of occipital hinge deformity are asymptomatic. The disease is often discovered incidentally through imaging in patients with other health problems.
1.2 Classification of Chiari . malformations
Chiari malformation type I This type of malformation occurs during fetal development, and is characterized by the cerebellar amygdala moving more than 4 mm below the occipital foramen into the cervical canal. This movement prevents the normal circulation of cerebrospinal fluid between the spinal canal and the intracranial space.
Patients with Chiari malformation type 1 often have abnormalities in the base of the skull and spine such as:
Compression of the upper part of the spine into the base of the skull, causing compression of the brain stem; Attach the body of the first cervical vertebra to the base of the skull; Partial adhesions of the 1st and 2nd cervical vertebrae; Klippel-Feil deformity (congenital adhesion of the cervical vertebrae); Hidden vertebrae; Scoliosis . Many patients with Chiari malformation type I are asymptomatic. Others have some symptoms related to root canal growth such as: Headache, severe neck; occipital headache, which is worse when coughing, sneezing, or straining; weakness in hands and arms; loss of pain sensation and temperature sensation of the upper body, arms; collapse due to muscle weakness; dizzy ; spastic paralysis; have problems with balance; double or blurred vision; Hypersensitivity to bright light.
Chiari malformation type II This type of malformation is seen almost exclusively in patients with medullo-meningoceles, characterized by downward movement of the medulla oblongata, cerebellum, and fourth ventricle into the cervical spinal canal. elongation of the pons and fourth ventricle.
Symptoms of type II occipital hinge deformity are: Change in breathing rate, vomiting, arm weakness, involuntary downward eye movement.
Chiari malformation type III This malformation includes congenital spinal malformation syndrome, herniation of part of the cerebellum and/or brain at the back of the head or neck. This is a rare malformation with a very high rate of early death or severe neurological disturbance in survivors.
Chiari malformation type IV This is the most severe and rarest type of occipital hinge malformation, characterized by the failure of the cerebellum to develop normally, with possible other brain and brain stem malformations. Most babies born with Chiari malformation type IV die prematurely.
Symptoms of Chiari malformation type IV are: Scoliosis; muscle weakness and spasticity; loss of sensation, especially hot and cold sensations; movement impairment; loss of bowel and bladder control; chronic pain; headache.
1.3 Diagnosis of occipital hinge deformity
Several methods help diagnose and determine the extent of Chiari malformation:
Recording of brainstem auditory potentials helps to check the integrity of the auditory conduction system, used to determine whether the brain stem is active good action or not; Myelogram: An X-ray technique of the spinal canal after the injection of contrast material into the cerebrospinal fluid. The lumbar puncture method allows the doctor to visualize the compression of the spinal cord or nerves due to the deformity of the occipital neck hinge; Computed tomography: Using X-rays to diagnose, help determine the size of the ventricles, show blockage. However, this technique is less effective in analyzing the posterior fossa or spinal cord; Magnetic resonance imaging: Uses strong magnetic fields and computer technology to create 3-D images of body structures. This technique provides accurate images of the brain, cerebellum and spinal cord, thereby helping the doctor to clearly determine the degree of Chiari malformation, distinguish the progression; Somatosensory potential recording: A method of recording the electrical activity of nerves involved in sensation, providing some information about peripheral nerves, brain and spinal cord function.

Chụp cộng hưởng từ giúp chẩn đoán dị dạng bản lề cổ chẩm
1.4 Treatment of Chiari . deformity
Treatment of occipital hinge deformity depends on the type of deformity, progression of anatomical changes, or disease symptoms. With Chiari malformation type I without symptoms should be treated conservatively. If the deformity is symptomatic or causes spinal hollow, surgery is usually recommended. Chiari malformation type II is treated surgically if the patient is symptomatic and uncomplicated with hydrocephalus. The aim of surgical treatment of occipital hinge deformity is to optimally decompress nerve tissue and restore normal cerebrospinal fluid flow around and behind the cerebellum.
2. Details of surgical methods of occipital hinge deformity
2.1 Indications/contraindications
Indications
Chiari I malformation with clinical manifestations
Contraindications
Patients unable to anesthetize; Patients with coagulation disorders.
Bệnh nhân rối loạn đông máu không được chỉ định phẫu thuật
2.2 Preparation
Personnel performing: Neurosurgeon, anesthesiologist, assistant,...; Equipment: Cranial surgery kit, machine drill, craniotomy drill, specialized microsurgery glasses for neurosurgery, skull fixation pins, artificial patches, biological glue, hemostatic materials, ...; Patients: Being examined and diagnosed with Chiari malformation, examining to detect co-morbidities and related diseases, sharing information on surgical purposes, implementation process; fasting the evening before surgery; use some more prophylactic drugs as prescribed; Medical record: Complete according to the general medical record form.
2.3 Surgical procedure
Position: The patient lies on his stomach, fixed on the frame; Anesthesia: Endotracheal anesthesia; Incision of the skin in a straight line, the center of which corresponds to the occipital foramen; Open the cranial fossa posterior fossa and occipital hinge: Dimensions from the occipital foramen to 3cm, from the midline to the sides, at least 1.5cm; Resection of the first cervical vertebra; Open the dura in an inverted Y shape and try to preserve the arachnoid; Perform dural shaping; Close the dura and incision in anatomical layers. Before closing the final suture, the intradural space should be filled with water to remove air and detect bleeding if present.
2.4 Post-operative follow-up and handling of complications
Patients are monitored within 24 hours after surgery in the neuro-resuscitation department to promptly detect surgery-related complications.
Monitor vital indicators: Blood pressure, respiration, pulse, temperature,...; Use prophylactic antibiotics, pain relievers; Monitor for focal neurological signs and detect complications early; Treatment with postoperative bleeding: Early detection when there are clinical signs, computed tomography to check if necessary and when there is an intracranial hematoma, it is necessary to treat early according to the lesion; Treatment with cerebrospinal fluid leak: Sew up the incision or re-operate to patch the fistula; Treatment of wound infection: Use antibiotics, change the bandage daily or surgically clean the infection; Patients should return to exercise soon from the 2nd day after surgery if possible to avoid complications due to prolonged lying. Patients may also wear a soft neck brace for several weeks after surgery.

Sau phậu thuật, người bệnh được theo dõi kĩ huyết áp, nhiệt độ
Vinmec International General Hospital with a system of modern facilities, medical equipment and a team of experts and doctors with many years of experience in neurological examination and treatment, patients can completely peace of mind for examination and treatment at the Hospital.
To register for examination and treatment at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register online HERE.
MORE
How many vertebrae does the human spine have? Spine with tumor: What you need to know Complications if fractures are not treated early