This is an automatically translated article.
The article is expertly consulted by a Doctor of Gastrointestinal Endoscopy - Department of Medical Examination & Internal Medicine - Vinmec Da Nang International General Hospital.The gallbladder is located in the right inferior hepatic fossa, the gallbladder fossa extends from near the right end of the portal to the inferior border of the liver. On sonographic transverse view, the gallbladder neck is located relatively fixed in the major interlobular fissure, between the right lobe and the medial segment. In longitudinal sonographic view, an echogenic major interlobar fissure can be seen between the gallbladder and the right portal vein in many people (approximately 70%). Currently, ultrasonography of the gallbladder is the leading imaging method in the evaluation of the gallbladder and biliary tract.
1. Ultrasound image of gallbladder
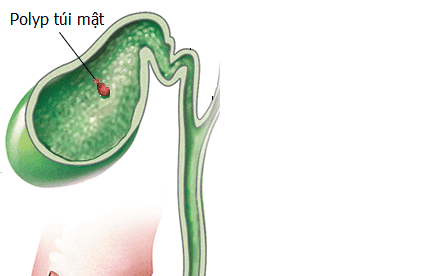
Recognizing the relationship between the gallbladder and the major interlobular branch is important, especially when the gallbladder is empty of fluid, or filled with stones or bile sludge. The gallbladder is divided into fundus, trunk, and neck. The fundus of the gallbladder is widest, the neck of the gallbladder is narrowest and connects to the cystic duct. Mucosal folds of the neck and cystic duct fold into spiral valves (Heister valves). The right wall of the gallbladder has a small pouch (Hartmann's pouch) that protrudes into the duodenum; However, this pocket is so small that the ultrasound cannot see it.On ultrasonography, the gallbladder is pear-shaped, filled with anechoic fluid. The normal gallbladder wall is echogenic and well-defined, with a thickness less than or equal to 3mm (≤3mm). The most accurate measurements are made of the anterior wall on the longitudinal axis when the sound wave beam is perpendicular to the gallbladder wall. Tilt transducer can cause false thickening of gallbladder wall. Normally, the gallbladder is 8 to 12 cm long. In adults, anteroposterior and transverse diameters measured on the longitudinal axis are less than or equal to 4 cm (≤ 4 cm).
2. Note when doing gallbladder ultrasound

Thông thường siêu âm có thể được thực hiện ngay mà không cần chuẩn bị
When performing an ultrasound of the gallbladder, the patient should fast before 8 to 12 hours because if eating, the gallbladder will shrink and make it difficult to examine, so it is possible to miss small lesions. However, in an emergency, the gallbladder can be ultrasounded without the patient having to fast. Usually use a cheap 3.5-5 MHz fan probe.
3. Gallbladder ultrasound technique
The usual investigation consists of scanning the patient's ribs in the supine or left-posterior position. Transcostal ultrasonography in the presence of intestinal gas ballooning. In addition, the ultrasound can be performed in the sitting or prone position, the prone position is more commonly used. The patient lies on the stomach, scans above the midaxillary line in the horizontal plane or the frontal plane, using the liver as an ultrasound window. The prone position is beneficial to demonstrate stone mobility, to avoid intestinal gas shadowing, to avoid echogenicity in a superficial gallbladder, and to reveal obscured stones in the neck of the gallbladder. Sometimes gallstones are only visible in the prone position.4. Ultrasound of gallbladder stones
Symptomatic gallbladder diseases caused by gallstones cause significant morbidity and mortality. The incidence of gallstones increases with age and risk factors such as obesity, rapid weight loss, bowel resection or ileal disease, elevated triglyceride levels, and ceftriaxone treatment. Gallstone components include cholesterol, pigment (calcium bilirubinate), or calcium carbonate. In gallstones, 90% of stones have mixed composition. Pure cholesterol stones make up 10% Calcium carbonate stones are rare, accounting for only 20% (between 10 and 40%) of stones that are calcium enough to be contrasted on plain film.
Các bệnh túi mật có triệu chứng do sỏi mật gây ra tình trạng bệnh và tỷ lệ tử vong đáng kể
For ultrasonography of gallstones, the patient is diagnosed as gallstone when there is an echogenic structure in the gallbladder lumen with echogenic shadow and moves in the patient's position. In diagnosing gallstones, the accuracy of ultrasound is as high as 96%. However, the size and number of stones in gallstones cannot be accurately assessed by ultrasound. Most gallstones produce a well-defined echogenic shadow (the shadow has clear edges and is free of acoustic or internal echo). In contrast, gastrointestinal gas proximal to the gallbladder produces an indistinct shadow with non-separate margins and echoes within the shadow, as well as echogenic noise. Most stones produce a clear shadow without echo because of attenuation (stones absorb most of the incident ultrasound). Only 20% to 30% of the ultrasound waves that reach the stone are reflected. In contrast, almost 99% of the incident ultrasound waves are reflected by the gastrointestinal tract, thus producing scattered and echoes posteriorly (indistinct shadow). However, some stones may produce an indistinct shadow because of the echoes diffused in the shadow, which is relative to the surface of the stone; Gravel with a smooth surface produces an indistinct shadow, while gravel with a rough surface produces a clear shadow.
The echo noise can be caused by calcified gallstones, cholesterol stones, and gas-filled fissured stones. Typically, calcified gallstones produce a strong acoustic shadow containing widely spaced echo bands and sometimes cometary tail noise (closed echo bands). In contrast, cholesterol stones (completely or largely) produce comet tail noises. Mud particles or small pieces of gravel containing cholesterol crystals can produce comet tail noises without shadowing.
The shadow is clearly visible when the stone is located in the center of the transducer, the center of the ultrasound beam, and is wide relative to the beam width and wavelength. For easier exposure of the acoustic shadow, a higher frequency probe or a closer focal probe is used, both of which narrow the ultrasonic beam width. Setting a high gain can blur the acoustic shadow by reducing the difference between the echo and adjacent tissue. The acoustic shadow may be more pronounced when the super beam is perpendicular to the gravel surface and weak or absent when the ultrasound beam is widely tangential to the gravel surface. Therefore, when there is hyperechoic structure in the lumen of the gallbladder especially when it is less than 5mm (<5mm) but no shadow is seen, take the following steps:
Decrease distal gain or global gain, Change angle between the transducer and the stone by slightly moving the transducer position or by ultrasound the patient in a different position. Ultrasound with a higher frequency transducer (5 instead of 3.5MHz) can create a shadow. Despite optimal technique, small stones, less than 3 mm in size, may not exhibit acoustic shadowing. In the case of not showing the shadow, it is necessary to take advantage of the blocking effect of many small stones that accumulate
Gallbladder ultrasound is an important part of the hepatobiliary screening package at Vinmec International General Hospital, performed by the team A team of highly qualified and experienced doctors in the field of screening for liver and bile diseases with the support of modern equipment and medical facilities will help accurately identify gallbladder-related problems.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.