This is an automatically translated article.
The article was written by Specialist Doctor II Pham Tien Ngoc - Emergency Department - Vinmec Central Park International General Hospital1. Investigation of excretory and detoxification functions
1.1. Bilirubin Bilirubin is a metabolic product of hemoglobin and heme-containing enzymes (95% from the degradation of red blood cells) Bilirubin TP: 0.8-1.2 mg% (5-17 μmol/L) Bilirubin GT (cockroaches) Next): 0.6-0.8 mg% (free, fat-soluble bilirubin, bound to plasma albumin, so not filtered through the glomeruli, when reaching the liver, bilirubin GT is conjugated with acid glucuronide to become glucuronide acid. bilirubin TT (conjugated bilirubin, water soluble, biliary excretion) Jaundice when Bil TP > 2.5mg%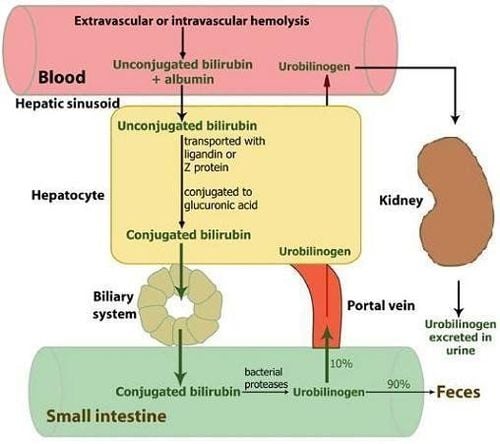
1.2. Urobilinogen A metabolite of bilirubin in the intestine, reabsorbed into the blood by the enterohepatic cycle, and then also excreted in the urine. Complete biliary obstruction will have no urobilinogen in the urine. Urobilinogen in urine is seen in cases of hemolysis (increased production), gastrointestinal bleeding, liver disease,... BT: 0.2-1.2 units (pp Watson). 1.3. Alkaline phosphatase (Alkaline phosphatase ALP) Origin: liver and bones (intestines, kidneys and placenta less). ALP bt: little thought to cause biliary obstruction. The half-life is about 7 days (increased ALP may persist for > 1 week, after biliary obstruction has subsided and when bilirubin has returned to normal). Increased ALP due to the liver is often accompanied by GGT and 5 ́- Nucleotidase Increase in ALP alone: liver disease caused by infiltration such as cancer, abscess, granuloma,... ALP increased 2 times bt: hepatitis, cirrhosis, metastasis , leukemia, lymphoma,... ALP increased 3-10 times: intrahepatic or extrahepatic biliary obstruction ALP not specific to the liver: increase in Paget's bone, bone resorption, bone metastasis, small bowel obstruction, pregnancy, children's bone growth... (5 ́- Nucleotidase) Low ALP: hypothyroidism, pernicious anemia, zinc deficiency,... 1.4. GGT (Ɣ- Glutamyl transferase) Although present in many other organs, GGT is found in high concentrations in columnar epithelial cells of the bile duct. The most common causes of elevated GGT alone: chronic alcoholism, biliary obstruction, drugs (acetaminopnen, phenyltoin), NASH (Nonalcoholic Steatohepatitis),... Half-life 7-10 days, but in chronic drinkers This period can be as long as 28 days. GGT is also increased in: renal failure, myocardial infarction, acute pancreatitis, diabetes, hyperthyroidism, COPD,... 1.5. Blood NH3 Produced: metabolized by bt proteins in the body and by bacteria living in the colon. The liver is responsible for detoxifying NH3, by converting it to urea, which is excreted by the kidneys. Skeletal muscle plays a role in detoxifying NH3, which binds with glutamic acid to form glutamine. Severe liver disease often results in muscle atrophy due to destruction, which contributes to elevated NH3. NH3 may be elevated in patients with severe portal hypertension or hepatic portal shunts. The concentration of NH3 in arterial blood is more accurate than in venous blood because it is not affected by NH3 from the intestine. NH3 can return to normal 48-72 hours before there is an improvement in neurological status.
2. Synthesizing function survey
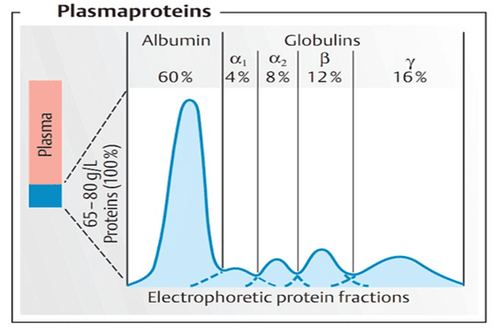
2.1. Blood Albumin The liver is the only place TH albumin is available to the body. Albumin maintains intravascular oncotic pressure and is a carrier of substances in the blood, especially drugs. Because of the great liver reserve capacity and the long half-life of albumin (about 3 weeks), serum albumin is reduced only in chronic liver disease or when liver damage is very severe. Cirrhosis ascites (decreased albumin due to escape into ascites), urinary loss of albumin (nephrotic syndrome), or gastrointestinal tract (chronic UTI). 2.2. Blood globulin: includes α1, α2, β, γ α1 Globulin (α1 antitrypsin, TBG, transcortin,...) α2 Globulin (haptoglobulin, ceruloplasmin, ....) β Globulin (β1 transferrin, β lipoprotein, ...) γ Globulin (immune antibodies) In cirrhosis, antigens from intestinal bacteria are not destroyed in the liver, but bypass the portal-host junction, creating an increased excitatory response in the reticuloendothelial system. , increases γ (IgG increases autoimmune hepatitis, IgM increases primary cholestatic cirrhosis,...) A/G < 1: cirrhosis, chronic hepatitis (decreased TH albumin, increased TH γ Globulin) di: Albumin 35-55g/L (55-60%)α1 Globulin 2-4g/L (4.2-7.2%)
α2 Globulin 5-9g/L (6.8-12%)
β Globulin 6-11g/L (9.3-15%)
Globulin 7-17g/L (13-23%)

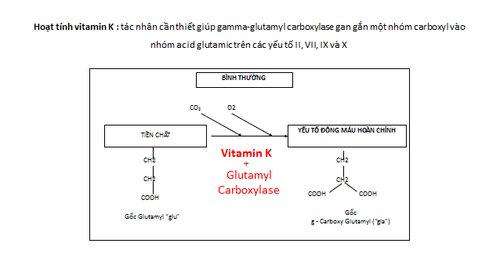
Vitamin K và các yếu tố đông máu sản xuất tại gan
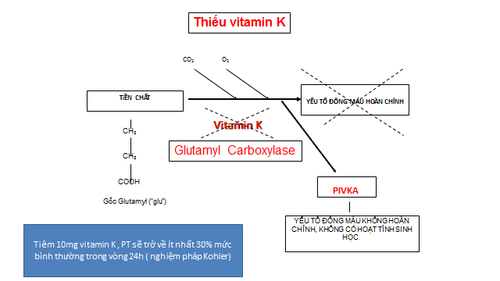
Liver disease: liver function declines in hepatitis, cirrhosis, liver K Vitamin K deficiency: due to diet (lack of substances: oil, fat, vegetables, beans, sesame, etc.). .), biliary obstruction, long bowel resection, long-term oral broad-spectrum antibiotics, vitamin K antagonists (coumarinic group). Malnutrition: patients suffering from gastrointestinal diseases (esophageal reflux disease, vomiting, coma, ... not eating or drinking for a long time will affect the coagulation system). placental abruption, stillbirth,..), surgery (multiple injuries, crushing, necrosis,...), internal medicine: gram (-), gram (+) sepsis, snakebite, transmission complications blood,... Fibrolysis (fibrinolysis)
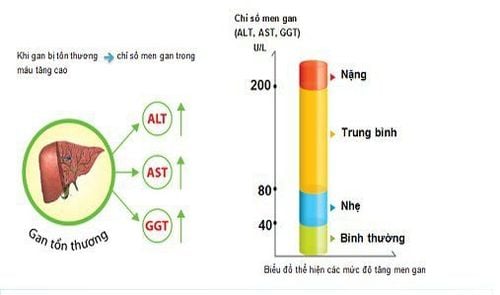
3. Test to assess the status of liver necrosis
3.1. Transaminase Intracellular enzyme, an increase in this enzyme reflects liver cell damage. AST: cardiac muscle, skeletal muscle more than in liver, in addition: kidney, brain, pancreas, lung, white blood cells, red blood cells. ALT: mainly hepatocyte cytoplasm. ALT bt: female: 19 UI/L, male: 30 UI/L Increased in most liver diseases, but not specific: myocardial infarction, rhabdomyolysis (myositis, muscular dystrophy), hypothyroidism, ... Artificial reduction: when there is increased blood urea. Elevated (>3,000 UI/L): hepatocellular necrosis, acute viral hepatitis, chronic, drug-induced liver damage, toxicity, prolonged vascular collapse (transaminase elevation has poor correlation with injury severity). Hepatocellular injury, and does not have much prognostic significance for example: very severe hepatocellular necrosis, liver enzymes are elevated for 24-48 hours, but after 3-5 days, enzymes decrease rapidly) Moderately ( <300 UI/L): alcoholic hepatitis, mainly increased AST (no more than 2-10 times ULN), possibly ALT bt or low (deficiency of pyridoxal 5-phosphate, Vitamin B6, cofactor for ALT synthesis in the liver) Increased mild (<100 UI/L): acute viral hepatitis, chronic liver disease (cirrhosis, chronic hepatitis, liver metastasis,...) or biliary obstruction, fatty liver. De Ritis Ratio (AST/ALT) O/P :
Tỷ số De Ritis ( AST/ALT) O/P
Tỷ số ALT/LDH
Evaluation of the liver's ability to work through liver enzyme tests Evaluation of bile function ; intravascular nutrition Early screening for liver cancer Perform tests such as Total blood cell analysis, blood clotting ability, screening for hepatitis B, C Assess hepatobiliary status through ultrasound images and other diseases risk of liver disease effects/exacerbation of liver disease.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.