
This is an automatically translated article.
The article was professionally consulted by Specialist Doctor II Cao Thi Thanh - Pediatrician - Pediatrics - Neonatology Department - Vinmec Hai Phong International General HospitalPremature babies in general face a wide variety of health problems, much of which depends on how preterm they were at birth. Lungs and breathing problems are always a top concern for premature babies.
1. Lung condition of premature babies
Premature babies are defined when babies are born before 37 weeks of gestation. Premature babies face a higher chance of developing one or more complications after birth.
One of the main concerns in premature babies is the lungs. The lungs of the fetus are complete and mature at 36 weeks, but the rate of development of each fetus is unique, no fetus develops like any other, so the time of 36 weeks is also indicative. relative. In general, if the risk of preterm birth is anticipated and where indicated, the pregnant woman should receive steroid injections before delivery to speed up lung maturation.
Trắc nghiệm: Thế nào là trẻ sơ sinh non tháng?
Trẻ sơ sinh non tháng rất cần được chăm và điều trị thật tốt để giúp giảm nguy cơ gặp phải các di chứng về tinh thần, vận động và sự phát triển sau này. Cùng theo dõi bài trắc nghiệm dưới đây để có thể nhận biết trẻ sơ sinh non tháng và có thêm kiến thức chăm sóc, nuôi dưỡng tốt nhất cho trẻ.The following content is prepared under supervision of Thạc sĩ, Bác sĩ y khoa, Ma Văn Thấm , Nhi , Phòng khám Đa khoa Quốc tế Vinmec Dương Đông(Phú Quốc)

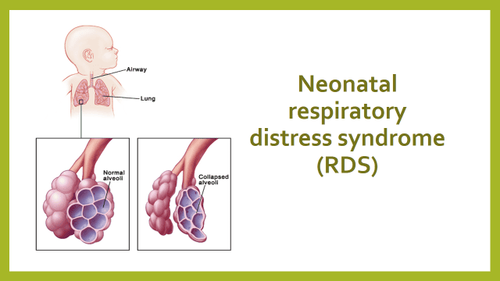
2. Respiratory distress syndrome (RDS)
One of the most common lung problems in premature babies is respiratory distress syndrome. The respiratory distress syndrome was formerly known as hyaline membrane disease (HMD).
Newborns develop respiratory distress syndrome when their lungs do not produce enough surfactant needed. Surfactant is a substance that helps reduce surface tension and stabilize alveoli, preventing alveolar collapse. Lack of surfactant in premature infants leading to respiratory consequences is inevitable. Chest X-ray of a child with respiratory distress syndrome shows diffuse opacities in the lungs.
Respiratory distress syndrome is very common in premature babies, because the fetal lungs usually do not start producing surfactant before the 30th week of pregnancy. Other factors that may increase the risk of developing neonatal respiratory distress syndrome include:
Racial factors (such as Caucasian) Gender male Family history Pregnant women with diabetes pregnancy
Hội chứng suy hô hấp (respiratory distress syndrome - RDS)
Respiratory distress syndrome tends to be less severe in infants whose mothers have been prescribed steroid injections before delivery.
Currently surfactant has been produced artificially, so in cases of infants lacking surfactant will be indicated to use. These children may still need additional oxygen support or ventilatory intervention.
3. Pneumonia
Pneumonia is an infection in the lungs that is caused by bacteria or viruses. Some infants develop pneumonia while still in utero, and require immediate treatment at birth.
Newborns can also develop pneumonia a few weeks after being born, and these cases are often complications of mechanical ventilation interventions (children are prescribed mechanical ventilation to resolve respiratory conditions such as respiratory distress syndrome or bronchopulmonary dysplasia).
The mainstay of treatment for pneumonia in preterm infants is to use antibiotics, consider adding oxygen support, or even requiring mechanical ventilation.

Trẻ sinh non dễ mắc một số bệnh lý về phổi
4. Apnea in premature babies
Another common breathing problem in premature babies is apnea. The pause in breathing causes the baby's heart rate and blood oxygen levels to drop.
Apnea occurs in virtually all babies born before 28 weeks of pregnancy. Babies born prematurely but after that point have a lower incidence of apnea, especially those born from 34 weeks of pregnancy on.
Apnea in preterm infants usually does not occur immediately after the baby is born, but often occurs after the baby is 1 to 2 days old, for infants who receive mechanical ventilation, sometimes when apnea does not become apparent until the child is weaned from the ventilator.
Apnea in preterm infants occurs for 2 main reasons:
The baby "forgets" to breathe, simply because the baby's central nervous system is not yet mature, and this is called central apnea. The baby is still trying to breathe normally, but the airway is obstructed so that ventilation cannot take place, and this is called mechanical obstructive apnea. Apnea in premature infants is often a combination of both.

Trẻ sinh non cần được hỗ trợ thở máy
Apnea in preterm infants is treatable. For central apnea, aminophylline or caffeine can be used, both of which stimulate the infant's immature respiratory system and reduce the number of apnea episodes. If the medication doesn't work, or if the apnea is too severe, the child will need mechanical ventilation until the child's nervous system matures. For purely mechanical obstructive apnea, the child is often intubated and mechanically ventilated to resolve the problem.
Apnea in preterm infants usually disappears when the baby reaches the age equivalent to 40 to 44 weeks of gestation (calculation is taken by taking the number of weeks of gestational age when the baby was born plus the number of weeks of the baby's age from the time of birth). born child). Sometimes the apnea goes away earlier, as early as 34 to 35 weeks of gestation. The child will not be discharged from the hospital until the child's condition is stable, in some cases the child's apnea does not completely disappear but persists, the child will only be discharged when the number of apnea episodes appears during the day. There are very few, and young parents will be instructed on the emergency operations of circulatory arrest as well as how to monitor and use medicine for the child.
5. Bronchopulmonary dysplasia
Bronchopulmonary dysplasia is a chronic lung disease, mostly seen in premature infants who need ventilators and oxygen therapy to intervene in acute respiratory disorders, but can also occur. in infants with less severe breathing problems.
Preterm infants, especially those born before 28 weeks of gestation, have very few alveoli in their lungs at the time of birth, and even those that have already formed are incomplete or inactive. function is as usual. For that reason, these children require respiratory support with oxygen or mechanical ventilation. Although medical interventions can help children survive, these same interventions can cause damage to the lungs, causing bronchopulmonary dysplasia to appear.
Because the number of active alveoli in children with the disease is very low, these children are forced to breathe much faster and more forcefully than normal healthy children. Most of the energy children use in breathing, the body has very little energy left to grow and develop, leading to growth retardation and inability to develop, leading to a series of problems in other organs of the body. body.
There is currently no specific treatment for bronchopulmonary dysplasia, but available treatments can help prevent, delay, or alleviate symptoms. Commonly used drugs include diuretics, bronchodilators, corticosteroids, and others, and severe cases of bronchopulmonary dysplasia will require additional oxygen support or mechanical ventilation.

Trẻ sinh non cần được chăm sóc đặc biệt
Most cases of bronchopulmonary dysplasia will get better gradually, although it will take time, and this time period will vary from child to child. In general, even after adulthood, children still have long-term effects from bronchopulmonary dysplasia, making them more likely to be hospitalized than other children.
Bronchopulmonary dysplasia is an unavoidable lung injury in premature infants if respiratory support is required. However, thanks to medical achievements, especially stem cell transplantation, this disease is no longer a long-term obsession. Vinmec Medical System has gradually applied and succeeded in not only nurturing premature babies but also preserving the child's respiratory function.
With many years of experience in examining and treating diseases in children, now the Pediatrics Department at Vinmec International General Hospital has become one of the major health care centers, capable of examining , screening and treatment of many specialized diseases in children. Therefore, if the child shows signs of poor absorption of nutrients, slow weight gain, growth retardation, etc., parents can take the child to Vinmec International General Hospital for examination and support. advice from qualified doctors.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
Articles refer to the source: healthline.com













