This is an automatically translated article.
Multifocal motor neuropathy (MMN) is a rare autoimmune peripheral neuropathy characterized by asymmetric motor weakness or reduction and muscle atrophy but no sensory abnormalities. sense.
1. Symptoms of multifocal motor neuron disease
Multifocal motor neuropathy has fairly obvious symptoms, specifically as follows:
Subacute onset with asymmetric weakness. Symptoms of lower motor neurone disease (LMN) usually present in a bilateral setting with arm and hand weakness without loss of sensation in other areas. Begins as a monofocal neuropathy affecting the distal arm; Wrist and hand weakness may also manifest in the legs. Often people with multifocal motor neuron disease begin to feel weakness in the arm, progressing often to spreading to the contralateral arm and then to the leg. Muscle tremors or cramps may occur. Muscle atrophy occurs late in the course of multifocal motor neuropathy. Deep tendon reflexes are significantly affected, reduced in most cases but normal or increased (but without pathology) in individuals with the disease. Cranial nerves, pharyngeal muscles, and respiratory muscles are often preserved in multifocal motor neuropathy. Nerve damage in multifocal motor neuropathy is variable, with some nerves unaffected, others severely damaged. Sensory conduction through the same nerve segment and cerebrospinal fluid protein is normal.

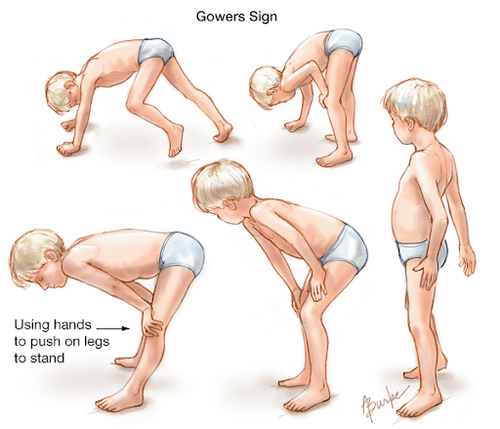
Teo cơ trên người bệnh dây thần kinh vận động đa ổ
2. Diagnosis of multifocal motor neuron disease
Diagnostic method for multifocal motor neuron disease.
Gradual or gradual progression, focal, asymmetric weakness, in the motor neuron distribution of at least two nerves, lasting more than one month. If symptoms are present only in the distribution of one nerve, only a "probable" diagnosis is made. There were no objective sensory abnormalities except for tuning fork-vibration abnormalities in the distal lower extremities. Clinical criteria supporting the diagnosis of the disease:
Mainly upper extremity weakness; Decreased tendon reflexes or loss of activity in the affected limb; There is no active involvement of the cranial nerves; Muscle cramps and tremors in the affected limb; Muscle strength response to immunosuppressive therapy; Differential diagnosis: same presentation but with scattered sensory lesions, called Lewis-Sumner syndrome or multifocal motor neuropathy and acquired multifocal demyelination. There is also motor neuropathy due to vasculitis.

Phản xạ gân xương bị giảm
Exclusion criteria:
Babinski (+) motor neuron signs (+), Hoffman(+); Have damaged pharyngeal muscles; Decreased sensation is noted more severely than distal lower extremity tuning fork fibrillation; Diffuse symmetrical motor weakness within the first weeks.
3. How to treat multifocal motor neuron disease?
Currently, there are quite a few methods of treating multifocal neuropathy, some effective treatment methods are as follows:
3.1. Treatment with Immunoglobulin Multifocal motor neuron disease is treatable with intravenous globulin, which is the first-line treatment in the treatment of multifocal motor neuropathy:
Possible plasma exchange with Activity is roughly comparable to that of immunoglobulins, which are excellent for short-term treatment of multifocal motor neurone disease, but they are generally ineffective and are not recommended for long-term repeat therapy. While Immunoglobulin is used in long-term repeated treatment. Most cases of multifocal motor neuron disease improve rapidly in muscle strength with immunoglobulin, but improvement is generally not sustainable after several months so an intravenous infusion of immunoglobulin is usually required every 2 to 6 months. the week. 3.2. Immunosuppressants In treatment-resistant cases, doctors may consider immunosuppressive medications. However, in some cases, corticosteroids do not work and sometimes even make the disease worse.

Điều trị bệnh thần kinh vận động đa ổ bằng thuốc
3.3. Plasma exchange Treatment of multifocal motor neuron disease with plasma exchange and Mycophenolate mofetil (Cellcept) has not been effective. The use of cyclophosphamide (Endoxan) and rituximab may be investigated.
Multifocal neuropathy has slow progression and defects in untreated patients, so before the disease leaves complications, patients should go to medical centers for examination and treatment.
To register for examination and treatment at Vinmec International General Hospital, you can contact the nationwide Vinmec Health System hotline, or register online HERE.
MORE:
Diagnosis and treatment of intercostal neuralgia Occipital neuralgia: The "culprit" that gives you headaches Common complications of trigeminal neuralgia