This is an automatically translated article.
Compared with the traditional method of opening the skull cap, the endoscopic approach to removing pituitary tumors brings more advantages to the patient, but this procedure is also difficult and complicated, requiring sophistication and precision. altitude body.
The entire procedure of laparoscopic pituitary resection through the sphenoid is presented in the following steps:
1. Preparation for pituitary tumor surgery
Magnetic resonance imaging and preoperative cranial computed tomography (CT) of the pituitary gland by transsphenoidal endoscopic method is essential for meticulous assessment of the size of the intranasal airways and detection of abnormalities. defects such as deviated nasal septum; learn the anatomy of the paranasal sinuses; structure of the pituitary tumor as well as the compression effect on the surrounding brain parts, especially the blood vessels that nourish the brain.
In cases of endoscopic transsphenoidal pituitary adenoma surgery due to tumor recurrence, the previously removed sphenoid sinus bone wall may be very fragile and lack a vascular stalk. However, the nasal septum can still be reused by preoperative imaging studies.
For recurrent pituitary tumors but small in size, without causing compression around, especially when the previously approaching sphenoid sinus has been damaged and difficult to recover, this treatment for pituitary adenoma is best done. through the opposite nostril.

Trước phẫu thuật, người bệnh bệnh được xác định vị trí khối u tuyến yên thông quan MRI sọ não
2. Prepare endoscopic equipment, patient and surgeon
2.1. Laparoscopic equipment preparation for pituitary tumor surgery 0 degree endoscope 18 cm range for nasal and sphenoid sinus stages 0 degree endoscope 30 cm range for pituitary access stage Endoscope 30 degrees and 45 degrees are used at the end of surgery to examine the tumor cavity and remove the remnants of the tumor. The outer sheath of the endoscope should be used to reduce the operative time, because it can Irrigation and cleaning of lenses. As a result, the movement of the endoscope in and out through the nasal cavity is significantly less than the Straight Clamp that holds the endoscope.
2.2. Preparation of the Patient Oxymetazoline Nasal Drops is instilled the night before surgery and then again in the morning before transferring the patient to the operating room. The patient is placed supine in the reverse Trendelenburg position, with the hips and knee flexed, raised 20 degrees The patient's head is kept in a central position, resting on a horseshoe-shaped headrest or fixed with a tripod headrest. Chin line or nose bridge is maintained parallel. parallel to the ground with the head turned 15 degrees toward the surgeon and tilted 15 degrees toward the opposite shoulder (with the left ear toward the left shoulder) The endotracheal tube is fixed to the left of the lower jaw and throat Tube nasogastric - gastric tube is placed to aspirate blood and secretions before extubating the patient Anesthetize the patient with propofol infusion to reduce bleeding, keeping blood pressure approximately 90 mmHg and pulse approximately 60 beats/min. Intranasal cavity can be placed in patients with large tumors with wide pituitary extension. To disinfect, use sterile cotton balls. n betadine instillation to clean the bilateral nasal cavity after determining the patient's position.

Tiến hành đặt ống nội khí quản cho người bệnh trước khi phẫu thuật
2.3. Prepare the surgeon Monitoring screen placed behind the patient's head Additional screen placed in front of the operating assistant The right-handed main surgeon stands to the right of the patient During the nasal stage, the surgeon Hold the irrigation and suction endoscopic handle in the left hand and the surgical instruments (drill, suction, curette, etc.) in the right hand The laparoscope holder or the position of the Mayo stand can be adjusted by the operating assistant as well as performing the operation. other suction manipulations in the nasal phase. At the same time, the assistant surgeon can also control the endoscope after reaching the tumor in coordination with the main surgeon Bio-glue and hemostatic device are always ready to use during surgery. . >>> Suggested article: Symptoms of pituitary tumor
3. The surgical process of pituitary tumor by endoscopic transsphenoidal method
Laparoscopic sphenoid surgery to remove pituitary adenoma consists of four stages. The outcome of each stage is the key to safe exposure for the next stages.
3.1. Nasal stage The endoscope is aligned with the floor of the nasal cavity and inserted in the midline of the septum. Infiltrate the nasal septum with two cotton swabs impregnated with five ampules of 1:1000 adrenaline diluted in 30 ml of 1% xylocaine . Hold in place for 5 to 10 minutes to allow the medicine to spread around. This is an important step to help create adequate space by clearing the nasal mucosa. Continue changing with other cotton pads and keep for 2 minutes to 5 minutes. It can be repeated from 2 to 3 times to help create a flap of the nasal mucosa easily, to limit bleeding and subsequent swelling and swelling.

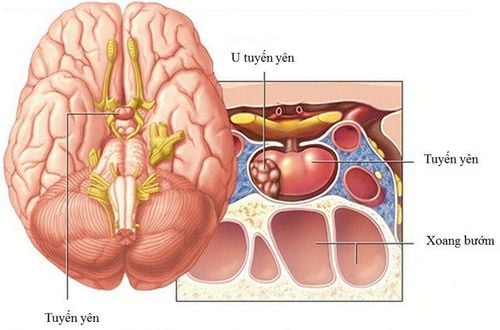
Phẫu thuật u tuyến yên thông qua nội soi đường xương bướm
3.2. Stage of the sphenoid sinus When the nasal passage to the sphenoid sinus is enlarged, the anterior sphenoid bone will be used with endoscopic tools to open the anterior wall and widen the septum of the sphenoid sinus. 3.3. Pituitary fossa phase The sphenoid sinus mucosa is located just above the anterior wall of the pituitary fossa. This septum is easily perforated with a bipolar electric knife to prevent stripping and prevent bleeding. The boundaries of the pituitary are confirmed in many directions with cranial locators or magnetic resonance imaging in the operating room Diamond burs are approached to open the pituitary floor by removing millimeters of the pituitary circumference until the pituitary gland is visible. The first exposed part is the sclera and is opened in several ways, which can be as follows: a vertical incision with diagonally enlarged sub-incisions, a cross-sectional incision, or two lateral longitudinal incisions joined by a central transverse cut When the sclera is opened, the pituitary tumor will be Full circumferential partial dissection to help remove the tumor in a single piece A multi-angle endoscope is inserted into the pituitary fossa to examine the tumor cavity to avoid missing tumor remnants Before the end of surgery During surgery, if remnants of the tumor are found, they are removed using a concave curved suction tube under direct vision. Use the 30 degree range. The angle range is located at 6 o'clock and these devices will be moved to the scope at 12 o'clock for a full view of the saddle at another angle, avoiding any hidden corners. Finally, check the whole thing. saddle fossa clockwise starting at 6 o'clock with the endoscope 30 degrees.

Hình ảnh mô tả thao tác bóc tách từng phần của khối u tuyến yên
3.4. Closing the incision After the tumor is removed, the surgeon prepares to close the sphenoid sinus wall. If necessary, a small skin incision is made in the abdominal wall to remove some of the autologous fat tissue to fill in the space left by tumor removal The hole in the wall of the sphenoid sinus will be replaced with a bone graft. nasal septum. However, synthetic grafts are sometimes used when a suitable septum piece is not available or the patient has had a previous laparoscopic pituitary surgery In addition, a bio-glue is used on the implant. Implants in the sphenoid sinus, help to heal quickly and prevent the leakage of cerebrospinal fluid from the brain parenchyma into the sphenoid sinus and paranasal spaces. Finally, a soft, flexible splint may be placed in the nose along the septum to control bleeding and prevent swelling. These splints also prevent adhesions that can lead to chronic nasal congestion.
In summary, with the benefits that endoscopy brings, sphenoid surgery by endoscopic pituitary resection is preferred over craniotomy. However, the patient needs to have a certain understanding of the steps in the above surgical procedure in order to have the best preparation, coordination with the doctors and a favorable surgery for himself.
Customers who have needs of examination and treatment can directly go to Vinmec Health System nationwide or contact for an appointment HERE.
Recommended video
Close-up of prostate cancer treatment with robotic laparoscopic surgery
In April & May 2021, when there is a need for examination and treatment of pituitary tumor at Vinmec Central Park International General Hospital, customers will enjoy double incentives:
- Free specialist examination
- 50% discount for customers with post-examination treatment indications. The program is limited to the corresponding technique of each hospital and to customers who perform this treatment technique for the first time at Vinmec.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.