This is an automatically translated article.
The article was written by Specialist Doctor I Vo Cong Hien - Doctor of Radiology, Department of Diagnostic Imaging - Vinmec Nha Trang International General Hospital.Cranial MRI is considered the most optimal noninvasive brain assessment method. Of particular value in the diagnosis of pituitary and brain stem disorders. Helps to detect and evaluate many diseases or abnormalities of the skull, especially brain tumors due to the clear and detailed images, observing the brain vessels without the need for contrast agent injection. Craniocerebral pathology is extremely diverse and complex, so it is necessary to follow a certain sequence to read the results of cranial MRI in addition to a specialist who has a thorough understanding of the knowledge and anatomy and imaging techniques to avoid missing lesions. .
1. Know the administrative information
Patient's name, age
Location to be taken:
Brain Pituitary and Cervical artery Indication
Technique:
Pulse type: T1, T2SE, T2 FLAIR, T2*, Diffusion and ADCmap, T1 gadolinium images .
Special case: Arterial and venous images: line, gado T1 IR, T2 CISS, T1 FS. Perfusion imaging, nerve bundle imaging, functional imaging, spectrometry. Cutting direction: cross section, forehead plane, vertical plane. Read images: Describe signs, explain based on location, anatomical structure, quantity.
a. Injury signature: Direct signature
Signal in each non-injection pulse sequence? Post-injection signal?
Result: Lesions: edema, solid lesions.
Hemorrhage, calcification, fat.

Hình ảnh MRI xuất huyết não tự phát
Brain lobe, midline, posterior fossa, base of skull... Is it compatible with clinical signs? Is the morphology and location consistent with the arterial perfusion area? Respect, not change the internal structure of the brain? Virchov Robin compartments unaffected? Single lesion or multiple lesions? b. Impact of injury on adjacent normal structures: Indirect signs.
Edema Pushing adjacent structures: cortical fissures, midline, intracranial plate... Brain recession: + Lesions on the tentacle: corpus callosum, temporal hook, cerebellar amygdala.
+ Posterior fossa: superior pupal lobe, cerebellar amygdala.
Ventricular dilation: + Due to blockage of CSF: blockage in the brain? or outside the brain?
+ Due to brain atrophy.
+ Due to the brain not developing: deformity.
Signs suggestive of etiology: depending on clinical history, other investigations, progress to read signs on magnetic resonance.
b.1. Lesions in the brain
Tumors in the brain: + Glioma: glioma
+ Nerve tissue: medulloblastoma, DNET
+ Hematopoietic tissue: lymphoma, retinoblastoma
+ Brain metastasis: Hematogenous , by the subarachnoid route.
+ Special cases: teratomas, intraventricular tumors, paraneoplastic syndromes.
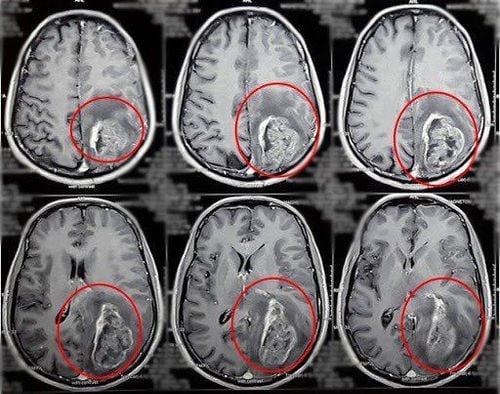
Hình ảnh u não thùy đỉnh - chẩm trái (vòng tròn đỏ)
Cerebrovascular accident : + Cerebral infarction : Arterial perfusion area, density and signal, etiology.
+ Hemorrhage of the brain, meninges.
+ Thrombophlebitis of cerebral veins.
Inflammatory diseases: multiple sclerosis, acute white matter disease, sarcoidosis... Infectious diseases: Bacterial infections: abscesses, pus accumulation, meningitis. Viral diseases: Herpes encephalopathy, HIV,... : Alcohol, drugs, carbon oxides... b.2. Extracerebral lesions: Tumor and pseudotumor / depending on location
Cranial: bone damage, focal or diffuse meningeal injury: meningitis. Base of skull: anterior layer, pituitary gland, midline, posterior fossa. c. Injury can be combined inside and outside the brain
Traumatic brain injury . Brain malformation, meningeal malformation, skull malformation: anterior cerebral malformation, allergen, lipoma, teratoma, Chiari. Arachnoid cyst, meningeal herniation. Connected to the skull joint. Neuro-dermal syndromes: Neurofibromatosis, Tuberous Sclerosis, Sturge Weber, Von Hippel Lindau... Of course multiple causes/possibilities could be discussed, certainty? Depending on the opinion of colleagues to have a solution: Urgent? Another visual survey? Other paraclinical investigations?

Hình ảnh u xơ thần kinh týp 1 trên phim chụp cộng hưởng từ
Vinmec International General Hospital is one of the hospitals that not only ensures professional quality with a team of leading medical doctors, modern equipment and technology, but also stands out for its examination and consultation services. comprehensive and professional medical consultation and treatment; civilized, polite, safe and sterile medical examination and treatment space.
Customers can directly go to Vinmec Health system nationwide to visit or contact the hotline here for support.