This is an automatically translated article.
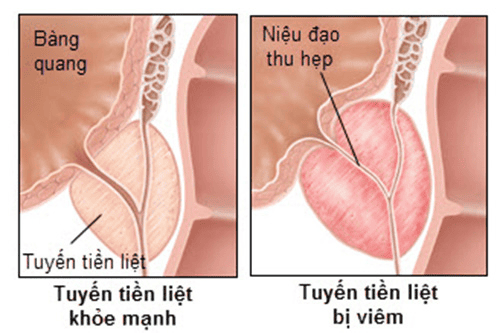
Posted by Doctor Hoang Tho - Department of Gastroenterology, Urology Surgery Robot & Pediatric Surgery - Vinmec Times City International General Hospital.The prostate gland is part of a man's reproductive system, located in front of the rectum and below the bladder, surrounding the urethra, through which urine exits. The prostate gland, along with the seminal vesicles, produces most of the fluid that comes out during ejaculation. During ejaculation, semen helps carry sperm out. Substances produced by the prostate gland and semen are important for reproduction.
1. Learn about prostatectomy
Patients with prostate cancer depending on the stage can be selected surgical removal of the entire prostate. It's called robotic-assisted total prostatectomy (RALP). Laparoscopic surgery is performed by injecting carbon dioxide into the abdomen so that a working cavity can be created. Through small incisions, the surgeon will place the Trocar through which the instruments are inserted into the abdomen. A small tube with a camera on the end is placed into one of the Trocar holes to help the surgeon see inside the body. Long thin instruments are placed in other Trocar holes to help your surgeon manipulate organs and perform surgery.
Robotic-assisted radical prostatectomy was first reported in 2001 by Dr. Gorbatiy, since then robotic prostatectomy has become one of the methods Optimal method to remove the entire prostate cancer. The robot system has 4 arms, one hand to hold the camera and 3 hands with attached tools. The surgeon controls all arms. The robotic arms are placed through the four Trocar holes to insert the instrument into the abdomen and an assistant surgeon will assist through the other trocar hole

Ung thư tuyến tiền liệt
2. How is the surgery done?
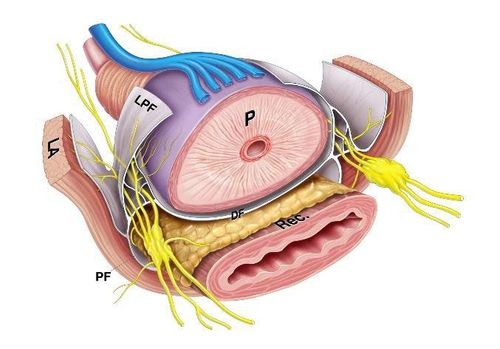
The surgeon will surgically separate the prostate from the bladder, remove the seminal vesicles and part of the sperm duct, and surgically separate the prostate from the rectum. After surgical removal of the entire prostate and seminal vesicles, the vas deferens, and the bladder neck will be sutured to the urethra, a small rubber catheter (sonde Foley) - will be placed from the urethra into the bladder. to promote wound healing and urinary drainage in the postoperative period. The removed prostate is sent for histopathology, which is carefully examined under a microscope.
A small drainage tube will be placed in the abdomen to drain the postoperative fluid after surgery. This tube is usually removed before you leave the hospital, but in some cases it can stay longer. In such a case, the doctor and nurse will instruct you on how to follow up and schedule an appointment to remove the catheter.
3. Control urination after surgery
The urethra is the tube that carries urine from the bladder through the prostate gland out. After the urethra exits the prostate, it passes through the striated urethral sphincter into the penile urethra and out, which helps control urine after surgery. After your surgeon has removed the prostate gland, the bladder is sewn to the urethra to restore urine flow. A small catheter will be placed through the penis and into the bladder to allow urine to flow freely into the bag.During the postoperative period, you will wear a catheter to help heal the wound. Your nursing team will teach you how to care for the catheter while you are in the hospital and discharged, the catheter is usually removed within 10-12 days.
After the catheter is removed, you will be taught to do a special exercise, called a Kegel exercise, which can help speed the recovery of urinary control. All men will have some loss of urinary control from the start. For most men, this improves quickly, within a few weeks. But there are some cases where it takes longer - a few months. By the end of the first year, more than 90% of men will have good urinary control.
4. Erectile Function
The nerves that control erection can also be affected during surgeries like RALP. These nerves only control the erection of the penis, and do not affect libido, frequency of intercourse, sensation in the penis.It is important to remember that full recovery of an erection can take up to 2 years . During this time, your urologist can offer you a variety of erectile dysfunction treatments (pills, injections, and vacuum devices), which can improve recovery. recovery of your erection and allows you to be sexually active during this active period.
Dây thần kinh kiểm soát sự cương dương của dương vật có thể bị ảnh hưởng trong quá trình phẫu thuật
5. Injury to the rectum
The rectum is another important organ located very close to the prostate gland. Rectal involvement very rarely occurs in <1% of patients.
Certain conditions such as previous surgery, hormone therapy, radiation treatment, infections, and other causes of scarring to the area can increase the risk of damage to the rectum.
If the rectum is damaged when it has been emptied before surgery, it can usually be sutured at the time of surgery without significantly altering your recovery
6. Bilateral pelvic lymph node dissection
Doctors may remove pelvic lymph nodes during your surgery. These small glands are located near the prostate and may be the first place prostate cancer spreads. This procedure takes another 20 to 30 minutes for your surgery. Vascular and nerve damage to this region is very rare with pelvic lymph node resection.
7. Invasive cancer cells
Some patients may have cancer that has spread beyond the gland that is not detected before or during surgery. This can be confirmed postoperatively, when tissue specimens are sent for pathology. The risk of invasion increases when prostate cancer is at an advanced stage.
Additional treatment (eg, radiation, endocrine, chemotherapy) after surgery may be needed depending on the stage of the disease, the invasive nature of the cancer cells, the presence of cancer in the seminal vesicles or lymph nodes.
8. Risk of surgery
Although robot-assisted radical prostatectomy is a minimally invasive surgery, it can cause complications like any surgery. These include:
Urinary tract infections Surgical site infections Injury to the bladder or ureters (very rare usually < 1%) Urinary fistulas due to vesicoureteral fistulas (risk <10%) may occur In addition, this may require a longer drain and also wear the catheter for a longer time. For most cases involving anastomosis, no further intervention is needed, as the body will heal itself with proper drainage. Sclerosing of the urethra at the junction of the urethra and bladder, sometimes requiring surgical removal of scar tissue (risk <5%) Permanent urinary incontinence - inability to control urine. This complication is very rare, occurring in less than 2% of patients. Erectile dysfunction (As described above) Rectal injury, rarely requiring colostomy, risk <1% Conversion rate to open surgery <2%. Swelling of the face and eyes, red pressure in the shoulders on both sides due to the surgical position you lie on the inclined surgical table, the low head and high leg position, this sign usually disappears the day after surgery.

Rối loạn cương dương
Complications related to anesthesia. Sore throat due to intubation (breathing tube). Bleeding may require blood transfusion (risk <10%). Extended intubation (holding a breathing tube longer after surgery if you can't breathe easily on your own). Usually this risk is higher in patients who smoke, have a history of emphysema (COPD), other lung diseases, sleep apnea, and are obese. Blood clots in a vein (especially in the legs or lungs). These can be life-threatening and often require long-term anticoagulation treatment. (<1% risk) Allergic reaction to the drug. Electrolyte (salt) imbalances may occur.
9. What if I am obese?
Robotic devices can reach the pelvis very well in most men, even those who are obese. However, we found a greater likelihood of complications in obese patients. These complications include an increased risk of bleeding, shortness of breath, urinary incontinence, blood clots, and pressure ulcers.
10. Device problems
Problems can occur with the robot machine, but it is a system with many built-in safety features to prevent the use of the machine in the event of a problem. In many cases we are able to correct these mechanical problems right away and proceed with the planned surgery. However, in a very few cases, we have to wait for an engineer to come to solve the problem, in such cases we will actively switch to open surgery to ensure patient safety.

Máy robot phẫu thuật
11. Brief overview
Patients undergoing robotic prostatectomy are as follows: The patient arrives at the hospital on the day of surgery, the surgery is then performed, and it usually takes 4 to 5 hours. After that, the patient is hospitalized for 3-4 days and is encouraged to exercise early and eat soon after surgery. Patients are discharged from the hospital with instructions for postoperative care and monitoring of urinary catheters and appointment of a follow-up visit.
Patient is prescribed outpatient treatment, Patient should exercise gently, avoid constipation, eat enough nutrients to improve physical condition.
The urinary catheter is removed for 10-12 days, after which, the patient can return to work within 2-3 weeks and then can return to unlimited activities in 3-4 weeks.
Up to now, Vinmec International General Hospital has successfully operated on digestive, urological - genitourinary and gynecological diseases with a success rate of up to 95%. Robotic surgery center is one of many steps of Vinmec Medical System, aiming to turn Vinmec Times City into a leading modern and comprehensive surgical center in Vietnam. Vinmec is successfully combining traditional surgical treatment (open surgery) and high technology (laparoscopic surgery, robotic surgery...), effectively helping to treat complex diseases.
To register for examination and treatment at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register online HERE.
MORE:
Robotic surgery "blows away" prostate cancer for Japanese doctors Why Robot Surgery is becoming a modern surgical trend? Holimum Laser Surgery - An advanced method of treating prostate enlargement