This is an automatically translated article.
The article was professionally consulted with MSc.BS Nguyen Huy Nhat - Department of Medical Examination & Internal Medicine - Vinmec Danang International General Hospital.Blind pleural biopsy is a technique with the aim of removing some pieces of the parietal pleura for histopathological examination. Blind pleural biopsy is indicated in case of exudative pleural effusion or blood red fluid.
1. Blind pleural biopsy
Blind pleural biopsy, also known as closed pleural biopsy, is a technique performed with the aim of taking some pieces of the parietal pleura for histopathological examination.2. Indications and contraindications
2.1 Designation
Blind pleural biopsy is indicated in cases of exudative pleural effusion or blood red fluid. In which pleural effusion is the phenomenon of appearing more fluid than normal physiological level in the pleural space, due to many causes and changes in clinical and X-ray. The amount of fluid in the pleural space is normally about 10-15ml.2.2 Contraindications
Coagulation disorder, hemostasis cannot be adjusted, when the test index shows: platelets < 90 G/l, Prothrombin ratio < 60% Hemodynamic disorders Severe cardiac arrhythmias Respiratory failure Chronic renal failure , acute renal failure
Bệnh nhân suy hô hấp chống chỉ định sinh thiết
3. Implementation steps
3.1 Preparation
Blind pleural biopsies are performed by doctors and nurses trained in pleural biopsies. In addition, some of the equipment needed to perform a blind pleural biopsy include:2 ampoules of atropine 1/4mg and 5 ampoules of lidocaine 2% 2ml Anti-shock kit. Syringe 5ml, syringe 20ml, needle 20G, needle.. N2 gauze: 2 packs. Transmission line: 1 set. Fork: 1 pc. Scalpel blade: 1 pc. Castelain biopsy needle set includes: cutting needle and specimen collection needle, a trocar set. Sample tubes for testing fluid: 5 tubes Formol container to preserve specimens after biopsies: 1. Petri dishes containing physiological saline for biopsy specimens: 1 pc. Fluid drainage tank: 1 pc. Sterile gloves: 2 pairs, clean gloves: 1 pair. Sterile razor.
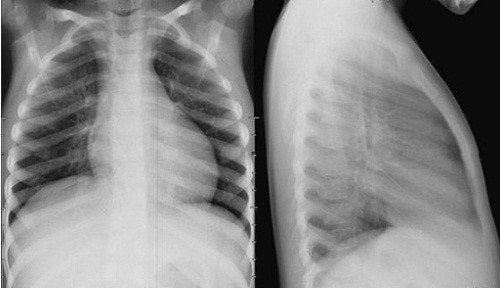
Trước khi làm thủ thuật, bệnh nhân cần chụp X-quang phổi
chest X-ray CT chest Ultrasound pleural blood test, basic coagulation.
3.2 Implementation steps
About 15 minutes before the procedure, the patient was injected subcutaneously with 1 ampule of atropine 1/4 mg. Place the patient in the equestrian position Locate the pleural biopsy. The biopsy site will be on the superior edge of the rib to avoid the intercostal nerve bundle. If this is the second biopsy, avoid the site where the first time was performed. Disinfect the area to be biopsied, and spread the hole. Anesthetize each layer of the chest wall, from the skin to the pleural wall. Avoid intravascular injection of Lidocaine. Then use anesthetic needle to probe the pleural fluid. Mark chest wall thickness. 500ml of 0.9% sodium chloride can be injected into the pleural space before biopsy for cases with little fluid. Place the set screw on the trocar so that the distance from the trocar tip to the screw is equal to the chest wall thickness plus 0.5cm. At the biopsy site, use the scalpel blade to make a small incision in the skin. Insert the trocar through the incision in a direction perpendicular to the chest wall. Withdraw the trocar barrel and attach a 20ml syringe to the trocar's sheath, aspirate, if fluid comes out, the trocar has entered the pleural space.
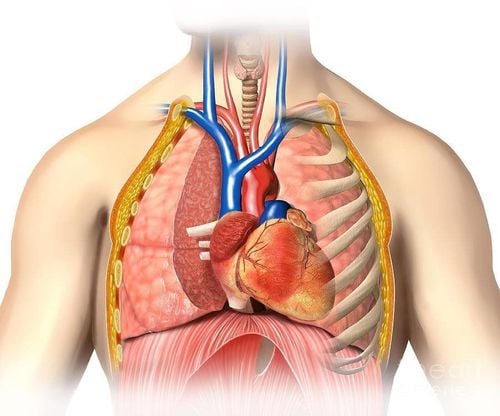
Sinh thiết màng phổi nhằm đưa trocar vào qua vết rạch qua thành ngực đi vào khoang màng phổi
4. Monitoring and handling complications
After the biopsy, the patient will be monitored in the ward. Some clinical symptoms such as fatigue, chest pain, sweating, subcutaneous emphysema, aspiration of a lot of air after biopsy, change in color of fluid if pleural bleeding is red, ..Some complications may occur during and after blind pleural biopsy such as:
Elevated vagal: the patient will feel tired, dizzy, slow pulse, low blood pressure. Need to stop the procedure, have the patient lie down, inject 2 ampoules of Atropin 1/4 mg intramuscularly and breathe oxygen through the nose. Continue to monitor pulse rate, blood pressure, and blood oxygen saturation. When blood pressure is <90/60mmHg, it is necessary to place a peripheral intravenous line immediately. Pneumothorax: there are symptoms such as chest pain, cough, shortness of breath,... The patient needs to have a straight chest X-ray. If the case of pneumothorax is less, give oxygen and monitor, or aspirate with a needle. If pneumothorax is large, pleural drainage is indicated. Hemothorax: the patient has symptoms of fatigue, chest pain, shortness of breath, blue skin, pale mucous membranes, rapid pulse, low blood pressure,... Perform pleural effusion to drain blood, transfuse red blood cells, Consult a specialist surgeon, monitor the amount of drainage > 300ml/hour for surgery.

Bệnh nhân có thể bị tràn khí màng phổi sau khi thực hiện sinh thiết màng phổi mù
Choosing the best blind pleural biopsy should choose large and reputable medical facilities not only in the general hospital system but also stand out, leading in the field of lung cancer diagnosis and treatment .
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.