This is an automatically translated article.
The article was written by a doctor at Cardiovascular Center - Vinmec Times City International General Hospital.When a heart valve has to be replaced, it means that the patient will trade "valvular heart disease" with another disease called "artificial heart valve disease". The ideal prosthetic valve should have characteristics close to that of a normal heart valve, have good hemodynamics, be durable, avoid the risk of thrombosis, and be convenient for cardiac placement.
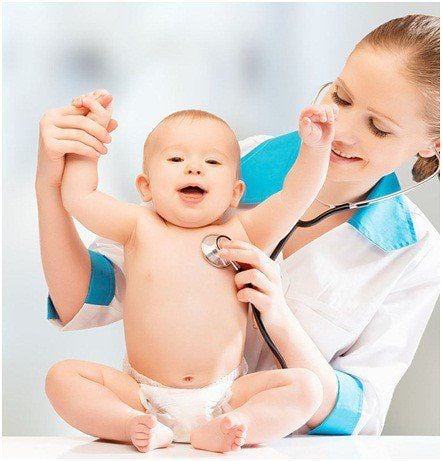
1. Types of artificial heart valves Mechanical valves Mechanical valves are made from artificial materials such as titanium, silicon... with a durability of 20 - 30 years or longer. Mechanical valves have very strong thrombolytic properties, so it is imperative to use anticoagulants of the vitamin K antagonist group permanently. There are three types of mechanical valves that have been used: ball valves, single-blade valves and double-bladed valves. In Vietnam, only 2-blade valves are in use. The valve consists of two semicircular valves attached to the rigid frame through a small hinge. The opening angle of the valve leaf relative to the valve ring plane is from 75° to 90°.
Các loại van cơ học: Van hòn bi (hình A), van 1 cánh (hình B và C) và van 2 cánh (hình D)
Types of biological valves:
Biological valves with brackets: The valve is designed like a human aortic valve. The valve can be made from a pig heart valve and then fixed on a Gutaraldehyde solution and then mounted on a metal and polymer support. Valve material can also be made from fixed bovine pericardium and mounted on the inside or outside of the holder. Bracketless biovalves: Manufacturers have attempted to increase hemodynamic efficiency and durability by eliminating the holder on biovalves. Percutaneous biovalves: Percutaneous aortic valve replacement is currently an alternative to conventional aortic valve replacement in patients with aortic stenosis who are at very high surgical risk or no longer have indication for surgery. The valve is attached to a device that is inserted through the skin into the ascending femoral artery attached to the aortic valve. In some cases, because of the small artery, it can be inserted through the small chest opening and then placed through the apex of the heart.

Van sinh học được tạo ra từ các mô động vật như bò, lợn, ngựa hoặc từ van của những người hiến tạng
Factors driving the selection of a mechanical valve The patient wants to use a mechanical valve and has no contraindications to long-term vitamin K antagonist anticoagulation. The patient has been indicated for long-term use of anticoagulants with vitamin K antagonists. The presence of a mechanical valve is only one risk factor for thromboembolic complications (eg, the patient already has atrial fibrillation). Patients with risk factors for increased biological valve degeneration (infancy, hyperparathyroidism or renal failure). Patients under 65 years of age and in good health. Factors leading to selection of biological valves Patients who want to use biological valves have been thoroughly explained about both types of valves. Patients cannot monitor the effects of anticoagulants well (in remote areas, ..) or because of work conditions, hobbies and do not want to use anticoagulants (such as football players, sports athletes). ..) The patient is over 65 years old or has a serious illness. Young woman who wants to have a baby. It should be further recommended that biological valves degrade more rapidly in young adults and during pregnancy. Selection of valve type and size This is the task of the cardiac surgeon. Doctors need to rely on long-term and reliable studies to choose the best valve for each patient.
With biological valves, the first factor to choose is the life of the valve. With mechanical valves, the first factor to choose is the low thrombus formation. The doctor will also choose the best hemodynamic valve to limit the disproportion between the size of the valve hole and the size of the patient. This phenomenon can be understood as the replacement of an artificial valve whose orifice area is too small for the patient to function normally and is more common in aortic valve replacement than in mitral valve replacement. . On ultrasound examination, after surgery will detect a pressure difference higher than the allowable level through the artificial valve, this can be considered as relative valve stenosis. In general, there are a number of factors that affect hemodynamics and thereby affect the disproportion between valve orifice size and patient size. From the same manufacturer, newer valves are better than older ones. Usually mechanical valves have better hemodynamics than biological valves. Valves located on the valve ring have better hemodynamics than those placed in the valve ring. Among biological valves, the unsupported type is hemodynamically better than the bracketed type (but the trade-off is a longer duration of cardiac arrest for surgery and a more difficult technique) Another very important factor when choosing a biological valve. Choosing the type of valve is a favorable factor for the surgical technique performed by the surgeon. Example: When replacing a mitral valve, preserving the posterior leaflet and all the ligaments is very important in eliminating the complications of cardiac rupture after valve replacement and improving cardiac function after surgery. The surgeon will choose which type of valve so that when replacing the valve, the ligaments and leaflets left behind will not obstruct or jam the artificial valve.