This is an automatically translated article.
The article was professionally consulted by Doctor of Urology Department, Vinmec Central Park International General Hospital.Laparoscopic nephrectomy is a modern technique, often applied to treat kidney cancer, or kidney failure. In laparoscopic nephrectomy, surgical instruments will be inserted through trocars in the intraperitoneal or retroperitoneal lines.
1. What is laparoscopic nephrectomy?
Laparoscopic nephrectomy includes: simple nephrectomy in benign non-functioning kidney disease, radical nephrectomy or resection of the whole kidney and perirenal fat into a mass in renal cell carcinoma, partial nephrectomy superior ureter or total ureter in urothelial cancer of the kidney or ureter and donor nephrectomy in kidney transplantation. Surgery can be performed via the intraperitoneal or retroperitoneal route. The kidney is removed in its entirety through a small lumbar slit or the specimen is chopped and removed through the trocar opening.2. In what cases is endoscopic nephrectomy indicated?
Laparoscopic nephrectomy is indicated in the following cases:● Benign kidney disease and loss of function, as determined by radioisotomy showing poor renal function (<10%) or diagnostic Imaging (CTScan) showed grade IV hydronephrosis. Common causes:
○ Hydronephrosis, loss of function due to ureteral stones, ureteral pyelonephritis.
○ Hydronephrosis without function due to congenital pathology: Narrowing syndrome
pyelonephritis - ureter, ureteral enlargement or vesicoureteral reflux.
○ Hydronephrosis lost function due to ureteral stricture after surgery.
○ Renal vessel hypertension: Renal artery stenosis, kidney atrophy.
○ Loss of function polycystic kidney disease.
● Cancer: Clear cell carcinoma of the kidney (RCC: T1 - T3a), transitional cell carcinoma of the renal pelvis or ureter (TCC)
● Endoscopic nephrectomy in a living donor for kidney transplantation .

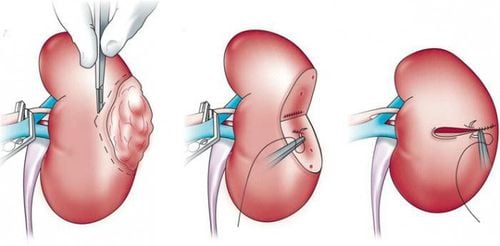
Mổ nội soi cắt thận trong trường hợp ung thư thận
3. Is laparoscopic nephrectomy dangerous?
Laparoscopic nephrectomy is an effective and safe treatment, with reduced blood loss, less postoperative pain, and faster recovery time than traditional open surgery. The incision is relatively small, aesthetic for the patient. This surgical method has many advantages, but it requires a system of modern equipment and supporting machines with high accuracy. Besides, the surgeon must also be a highly skilled person to avoid complications.4. How does laparoscopic nephrectomy take place?
4.1. Preparation ● Basic tests and assessment of residual renal compensatory function.● Abdominal ultrasound, computed tomography of the urinary system with contrast to determine pathological causes and evaluate bilateral renal function. A retrograde uretero-pyelogram may be needed if necessary.
● Radioisotope scan to determine the function of each kidney, percentage decrease or loss of function of the pathological kidney.
● Doppler ultrasound of renal blood vessels, renal angiography to identify hypertension due to atrophy and narrowing of renal arteries.
● Prepare for surgery as prescribed.
4.2. Performing surgery Laparoscopic renal surgery is performed through the following main steps:
Step 1: Position
The patient is tilted 75° for transperitoneal laparoscopic surgery and 90° inclined for retroperitoneal laparoscopic surgery. fascia, padded below the lumbar rib on the opposite side.
Step 2: Anesthesia
The patient is given endotracheal anesthesia, nasogastric tube placement, urethral catheterization.
Step 3: Select the location and place the trocar
In laparoscopic surgery, instruments are inserted into the abdomen through the trocar. In laparoscopic nephrectomy, trocar locations can be selected in:
● Transperitoneal route: For the right side use 4 trocars, the left side use 3 trocars. Open the small peritoneum and place the first trocar l0mm at the position next to the umbilicus, this is the camera position with the 30 degree lens. The remaining trocars include 2 l0mm trocars at position
above the iliac crest and below the costal margin, and 1 trocar 5mm in the midline between the umbilicus and the sternum.
● Retroperitoneal line: Trocar 1: 10mm was placed by the open method in the position above the iliac crest above the mid-axillary line to use the camera with a 30° lens. Trocar 2: 10mm at the lower end of rib XII. Trocar 3: 5mm above the anterior axillary line
so that the 3 trocars merge into a triangle. A fourth trocar (5mm) can be added above the anterior axillary line, below the costal margin.
Step 4: Create retroperitoneal space
Make 1cm skin incision at trocar 1 position, use Pince to separate the muscle fascia into the SPM cavity, insert the self-made balloon with a gloved finger and 400-600ml of air to expand. Place subsequent trocars using a wide surgical instrument.
Step 5: Nephrectomy
● Transperitoneal laparoscopic nephrectomy
For right nephrectomy: Open the posterior peritoneum, push the colon and duodenum in the middle, lift the liver up. Dissect the ureter from the genitourinary vessel to the lower pole of the kidney and the hilum. Exposing the anterior aspect of the inferior vena cava and the renal vein, the renal artery lies posterior to the segregated vein.
For left nephrectomy: After opening the left longitudinal fascia of Toldt, cutting the splenic-colon ligament, the spleen and left colon are pushed inward, releasing the lower pole of the kidney, the ureter and exposing the renal artery and vein. Arterial dissection, clip hemolock and dissect the artery first, then clip hemolock, dissect the vein.
Simultaneously clip the left adrenal vein and the left genital vein to drain into the renal vein. The kidneys are released to the upper, lower, and posterior poles. The ureter is released, clipped, and cut low. Intra-abdominal pressure was reduced to less than 5 mm Hg to check for bleeding in the surgical site and the pedicle resection process. Specimens were chopped
in the endoscopic bag and removed through the trocar hole.
Retroperitoneal laparoscopic nephrectomy Open the Gerota fascia, dissect, push the peritoneum forward and into the perirenal fat layer. Dissection through the lower pole to expose the ureter up to the renal hilum, expose the inferior renal pole, posterior and anterior surfaces, and then expose the superior renal pole.
Push the kidney forward and expose the renal peduncle, or follow the left genital vein to find the renal vein. Dissection of fat layer anterior and posterior renal peduncle. If you go to the back, you will reveal the first renal artery, if you do the anterior dissection, the first renal vein will be exposed.
Clip, hemolock and anterior renal artery ablation.
Renal vein can be forced to strengthen with thread when clip to reduce diameter, and cut loose. Expose the accessory renal arteries and veins entering the renal hilum and the renal poles and veins entering the renal poles and adrenal glands.
Release around the kidney and ureter, clip the ureter down low, cut the whole kidney, stop bleeding from the vascular branches originating from the lumbar muscle mass and the vessels in the perirenal fat layer by electrocautery or 5mm clip.
Reduce inflatable pressure to 5-10 mmHg, carefully detect bleeding points in common locations such as genital veins, renal peduncles, adrenal glands, and ureterectomy apex. Specimens are put in a plastic bag, taken through the first trocar.
Notes for nephrectomy for transplantation
Renal peduncle is paired, the vein can be cut first, then the artery is removed. The kidney is taken out in its entirety through a small opening in the abdominal wall connecting the first two trocars, or after laparoscopic surgery, the anterior abdominal wall and kidney peduncle are opened, then cut apart and taken out.
4.3 Monitoring and managing complications Some complications can be encountered:
● During surgery: Peritoneal tear, pleural tear, diaphragm perforation, bleeding due to vena cava injury,...
● After surgery, there may be intra-abdominal bleeding, fluid accumulation or residual abscess in the abdomen..
Therefore, monitoring and management of complications is done both during and after surgery.
5. Endoscopic partial nephrectomy at Vinmec Central Park International Hospital

Bệnh viện Vinmec Central Park có những chuyên gia hàng đầu về tiết niệu
Specialist Doctor II Nguyen Minh Quang Master Doctor Nguyen Tan Cuong Department of Urology at Vinmec has successfully performed many laparoscopic and open surgeries to treat emergency diseases of gastrointestinal - hepatobiliary; orthopedic; Urology surgery....The hospital is equipped with a system of modern and advanced machines such as: Gastrointestinal endoscopic surgery machine, C-ARM, arthroscopic surgery machine to help support doctors in the field of urology. surgical process.
To register for examination and treatment of kidney and urinary problems at Vinmec Central Park, you can register here or contact hotline 0283 6221 166 for support.