This is an automatically translated article.
This article was professionally consulted by Specialist Doctor I Truong Nghia Binh - Obstetrician-Gynecologist - Department of Obstetrics and Gynecology - Vinmec Da Nang International General Hospital. Doctor has more than 13 years of experience in the field of Obstetrics and Gynecology.It is estimated that 1 in 7 pregnant women experience gestational diabetes. Not only adversely affects the health of the mother, gestational diabetes also harms the development of the fetus. Testing for gestational diabetes is the most effective way to control this condition. The following article will help you get more useful information about gestational diabetes.
1. What is gestational diabetes?
According to the definition of the World Health Organization (WHO), gestational diabetes (or gestational diabetes) “is a state of impaired glucose tolerance of any degree, with onset or first detected during pregnancy". This condition often has no symptoms, so it is difficult to detect and will disappear after 6 weeks from birth.Subjects at high risk of gestational diabetes:
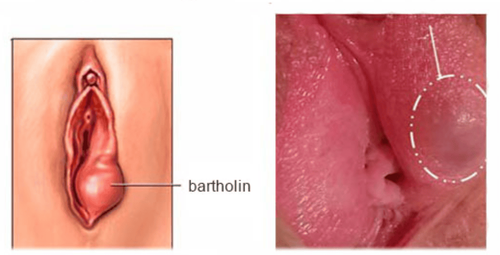
Overweight, obese. Family history: Someone with diabetes, especially someone with first-generation diabetes. Birth history ≥ 4000g. History of abnormal glucose tolerance including previous history of gestational diabetes, positive urine glucose. The older the age, the higher the risk, ≥ 35 years old is a high risk factor for gestational diabetes. Abnormal obstetric history: unexplained stillbirth, unexplained recurrent miscarriage, preterm birth, fetal malformation. Race: Asians are at high risk for gestational diabetes. Polycystic ovary syndrome. Gestational diabetes accounts for 3-7% of all pregnant women, poses many risks to the mother and fetus if not properly monitored and treated.

Bệnh tiểu đường thai kỳ chiếm từ 3-7% tổng số phụ nữ mang thai
2. Is gestational diabetes dangerous?
2.1 Effects on the mother Pregnant women with gestational diabetes may have an increased rate of miscarriage, stillbirth, premature birth, high blood pressure in pregnancy, polyhydramnios, urinary tract infections, pyelonephritis , cesarean section. In the long term, pregnant women with gestational diabetes have an increased risk of developing type 2 diabetes and related complications, especially cardiovascular complications. Pregnant women with gestational diabetes have a higher risk of complications during pregnancy than normal pregnant women. The common complications are:High blood pressure Pregnant women with gestational diabetes are more prone to hypertension than normal pregnant women. High blood pressure in pregnancy can cause many complications for the mother and the fetus such as: preeclampsia, eclampsia, cerebrovascular accident, liver failure, kidney failure, intrauterine growth retardation, premature birth and increased perinatal mortality. The proportion of pregnant women with gestational diabetes with preeclampsia is about 12% higher than that of women without gestational diabetes. Therefore, measuring blood pressure, monitoring weight, finding proteinuria regularly for pregnant women with gestational diabetes is essential in every routine prenatal check-up
Preterm birth Pregnant women with gestational diabetes increased risk of preterm birth compared with women without gestational diabetes. Causes of preterm birth are delayed glycemic control, urinary tract infection, polyhydramnios, preeclampsia, and hypertension.
Polyhydramnios Heavy amniotic fluid usually begins to be seen between the 26th and 32nd weeks of pregnancy. Excessive amniotic fluid also increases the risk of preterm birth in pregnant women.
Miscarriage and stillbirth Pregnant women with gestational diabetes have an increased risk of spontaneous abortion, pregnant women with recurrent miscarriages need to have their blood glucose checked regularly
Urinary tract infections Pregnant women with diabetes If gestational diabetes is not well controlled, the risk of bacteriuria increases. Urinary tract infections may be asymptomatic, but they cause a woman's plasma glucose to become unbalanced and require treatment. If not treated, it will easily lead to acute pyelonephritis, thereby causing many other complications such as ketosis, preterm birth, amniotic fluid infection
Long-term effects Many studies have found that, Women with a history of gestational diabetes have an increased risk of developing type 2 diabetes in the future. In addition, pregnant women with gestational diabetes have an increased risk of developing diabetes in subsequent pregnancies. They are also prone to obesity, excessive weight gain after giving birth without proper diet and exercise.
2.2 Effects on the unborn baby
Hiện tượng thai tăng trưởng quá mức là hậu quả của tăng vận chuyển glucose từ mẹ vào thai
Excessive growth and large fetus Phenomenon of excessive fetal growth is the result of increased glucose transport from the mother to the fetus. This amount of glucose has stimulated the pancreas of the fetus to secrete insulin, increasing the energy requirements of the fetus, stimulating the development of the fetus.
Hypoglycaemia and metabolic diseases in the neonate Occurs about 15% - 25% in neonates of gestational diabetes with diabetes. The cause is usually due to the fetal liver's poor response to glucagon, causing decreased gluconeogenesis from the liver.
Respiratory pathology: Critical respiratory syndrome. Previously, neonatal critical syndrome was the leading cause of death, accounting for 30% of neonates of gestational diabetes mellitus. Currently, this rate is about 10% thanks to the means of assessing fetal lung maturity.
Mortality immediately after birth Erythrocytosis is a common condition in neonates of pregnant women with gestational diabetes.
Neonatal jaundice Increased hemoglobin destruction leads to increased plasma bilirubin causing neonatal jaundice, which occurs in about 25% of pregnant women with gestational diabetes.
Long-term effects Increasing the prevalence of obesity in children, early childhood onset of type 2 diabetes as adults, and psychomotor-motor disorders. Babies born to mothers with gestational diabetes have an 8-fold increased risk of diabetes and prediabetes between 19 and 27 years of age.
3. How to detect gestational diabetes?
Women at high risk for gestational diabetes should have a gestational diabetes test, also known as an oral glucose tolerance test. This is the method used in the diagnosis of prediabetes and diabetes, especially to detect gestational diabetes, performed between 24 and 28 weeks of gestation.
Xét nghiệm tiểu đường thai kỳ là biện pháp hữu hiệu nhất giúp phát hiện tiểu đường thai kỳ
Steps to perform a 1-step test of 75 grams of Glucose (with venous blood)
Visit 1: When a pregnant woman comes to the clinic for the first time in the first 3 months of pregnancy, test fasting plasma glucose or blood glucose any similarity. If abnormal fasting plasma glucose is ≥ 126 mg% or any plasma glucose is ≥ 200 mg%. Diagnosing diabetes, referral to endocrinology. Follow-up visit: When the pregnancy enters the 24-28 week, advise pregnant women on screening for gestational diabetes, distribute leaflets with information related to gestational diabetes and guide to appropriate eating. It is reasonable to perform a glucose tolerance test of 75 grams - 2 hours at the next routine antenatal visit, note in the antenatal check-up the date of the follow-up visit with the plasma glucose test in red ink for easy recall. Some notes when performing a blood sugar test:
Three days before the diagnostic test, do not eat a diet with too much glucid and do not abstain too much to avoid affecting the test. Fasting for 8-12 hours before the test. Take 2ml of venous blood and measure fasting plasma glucose before testing. Drink a glass of sugar water that has been prepared by a medical facility and drink within 5 minutes. Take 2ml of venous blood, measure glucose in plasma at 2 times of 1 hour and 2 hours after drinking glucose water. During the test, the pregnant woman can't eat or drink anything, sit and rest in the testing room, or walk lightly around the hospital grounds during the test. The Maternity Package at Vinmec International General Hospital helps customers complete antenatal check-ups and necessary tests during pregnancy, including screening tests for gestational diabetes. Customers registered for Maternity Package are fully cared for and checked for health of mother and baby before birth - during childbirth and after birth, fully and conscientiously.

Hình ảnh khách hàng được tư vấn sức khỏe sau khi khám thai tại Vinmec
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.