This is an automatically translated article.
The article is professionally consulted by Doctor Department of Medical Examination & Internal Medicine - Vinmec Hai Phong International General Hospital.
Classification of acute cholecystitis is divided into 3 levels: mild, moderate and severe depending on the actual clinical situation. Diagnosis of acute cholecystitis is based on clinical examination, laboratory work, ultrasound, computed tomography and scintigraphy. Most cases of acute cholecystitis are caused by gallstones.
1. Classification of cholecystitis grades
Currently, the classification of acute cholecystitis is widely applied as follows:
Mild acute cholecystitis (grade 1): The gallbladder is mildly inflamed, inflammatory reactions appear locally. The patient is relatively healthy, without organ dysfunction; Moderate acute cholecystitis (grade 2): Gallbladder inflammation, accompanied by one or more of the following criteria: WBC > 18 g/L, palpable mass in the right upper quadrant, disease duration > 72 hours , with local inflammatory lesions, such as biliary peritonitis, gallbladder abscess, liver abscess, gallbladder necrosis. Severe acute cholecystitis (grade 3): The gallbladder is inflamed, with dysfunction in one or more organs, including cardiovascular function (hypotension), neurological, respiratory, and functional functions. renal, hepatic, hematologic disorders, (platelet count less than 100,000/mL).

2. Diagnostic criteria for acute cholecystitis
2.1. Clinical symptoms Abdominal pain: The main symptom of uncomplicated acute cholecystitis is colic in the liver, caused by the obstruction of the gallbladder neck by stones. There are 72-93% of patients with signs of right upper quadrant pain and epigastric pain combined, followed by nausea and vomiting. Fever: The number of cases of acute cholecystitis with fever is not high, patients with fever > 38oC are only seen in about 30% of cases. Half of the patients have abdominal wall reaction, rarely palpable mass in the right upper quadrant. Peritoneal reactions and spasticity of the abdominal wall are relatively rare. Murphy's sign: To identify Murphy's sign, the doctor places the fingertips of the right hand on the lower area of the patient's right flank and asks them to exhale, this time the doctor presses the hand deeper, when When the patient breathes in, the hand stays still. After 3 - 4 times like this, if inhaling, the patient suddenly stops breathing because of pain is a positive Murphy sign, this happens because of touching the patient's inflamed gallbladder. Murphy's sign has been widely used as a diagnostic factor for acute cholecystitis. The drawback of Murphy's sign is that the definitive diagnosis of acute cholecystitis can be concluded as soon as the Murphy sign (+), but in the case of Murphy (-), does not mean that the patient does not have pouchitis. level secret.
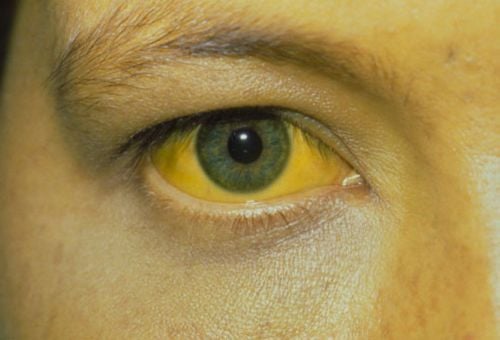
2.2. Laboratory Tests There is no specific blood test in the diagnosis of acute cholecystitis. However, the presence of infection is suggestive to supplement the diagnosis. Accordingly, leukocytes and CRP were increased, with a slight increase in serum enzymes in the hepatobiliary system and bilirubin.
In which, the bilirubin level can increase to 4 mg/dL (corresponding to 68 μmol/dL) in uncomplicated cases. In the case of ultrasonography showing acute cholecystitis and an increase in CRP > 3 mg/dL, the diagnosis of acute cholecystitis has a sensitivity of 97%, specificity of 76% and a positive predictive value of up to 95%.

2.3. Ultrasonography Ultrasound is the preferred method for first use in cases of suspected acute cholecystitis.
The diagnosis of acute cholecystitis due to gallstone formation by ultrasound is confirmed when the physician observes: gallbladder wall thickening (from 5 mm or more), fluid surrounding the gallbladder, or pain when Press the transducer directly to the gallbladder site (Murphy's sign on ultrasound). In addition, the gallbladder is enlarged, gallstones are present, echogenicity and gas image are present.
However, due to differences between different reports in terms of sensitivity and specificity, the diagnosis of acute cholecystitis should be made after comprehensively synthesizing the individual results.
There are many imaging methods that allow doctors to visualize gallstones. However, which technique to use must be carefully considered on a case-by-case basis.
Patients with cholecystitis can go to Vinmec International General Hospital for examination and treatment. There are full technical facilities as well as professional qualifications to effectively implement methods to accurately diagnose the degree of cholecystitis. The team of doctors with expertise in Gastroenterology at Vinmec are well-trained and experienced, a complete and modern medical equipment system and professional service quality will bring effective diagnosis and treatment. highest value.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.