This is an automatically translated article.
Article written by Master, Doctor Mai Vien Phuong- Gastrointestinal endoscopist - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital
Gastrointestinal fistula is a connection from the intestine to other nearby organs of the intestine or to the outer skin surface. In fact, this is the abnormal exit of digestive juices into another organ. It often develops secondary to abdominal trauma, infection, surgical procedure, or some underlying inflammatory disease process. Gastrointestinal fistulas require surgical treatment in combination with antibiotic therapy.
1. Overview of the digestive system
The digestive system includes the alimentary canal and digestive glands. The digestive tract includes the mouth, teeth, pharynx, tongue, esophagus, stomach, duodenum, small intestine, large intestine, appendix, and anus. Digestive glands include salivary glands, bile glands, pancreas, and intestines. This is the most important part of the body that helps to break down food for easy absorption and metabolism by the body. The salivary glands are like a mixer, helping food pass down the esophagus and stomach more easily.
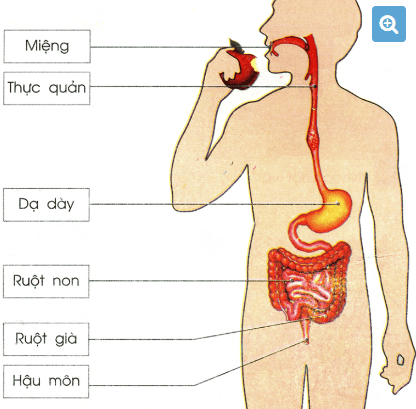
Hình 1: Hệ tiêu hoá con người
Hình 2: Hệ tiêu hóa – nơi xảy ra nhiều bệnh lý tiêu hóa phổ biến
2. Definition of gastrointestinal fistula
Fistula is an abnormal connection between two epithelial surfaces. Epithelial surfaces are present in hollow structures (such as blood vessels and organs) and include skin surfaces. Gastrointestinal fistulas are connections from the intestine to other nearby organs, other parts of the intestine, or external skin surfaces. In simple terms, a gastrointestinal fistula is an abnormal exit of digestive juices into another organ.
Gastrointestinal fistulas often develop secondary to abdominal trauma, infection, surgical procedure, or some underlying inflammatory disease process. Gastrointestinal fistulas can cause pus and digestive juices to leak to the outside of the body or to the connected organs through small sinuses. This can lead to infections and other complications. Gastrointestinal fistulas often require surgical treatment in conjunction with antibiotic therapy.
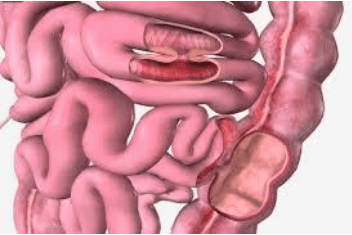
Hình 3: Dò ruột non – ruột non và ruột non – đại tràng
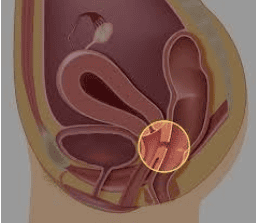
Hình 4: Dò trực tràng – âm đạo
3. Classification of gastrointestinal fistulas according to the location of the fistula
3.1. Leakage from digestive organs to skin
Fistula between parts of the small intestine (duodenum, jejunum or ileum) and the surface of the skin. Can be identified by percutaneous gastrointestinal leaks.

Hình 5: Hình ảnh rò đại tràng ra thành bụng
3.2. Fistula between different segments of the gastrointestinal tract
Fistula between two different segments of the intestine. Symptoms depend on the segment of the bowel that is leaky. In some patients no symptoms but may lead to malabsorption, diarrhea, dehydration.
3.3. Gastrointestinal fistula with bladder
Fistula between bowel and bladder. The colon, rectum, ileum, and appendix are all likely to form fistulas with the bladder. The large intestine is the most common, and is more common in male patients because they do not have a uterus to separate the two organs. Symptoms include pain, difficulty urinating, urinary incontinence, and smelly urine. To make a diagnosis, a person may have a urine sample, ultrasound, and other tests to locate the leak.
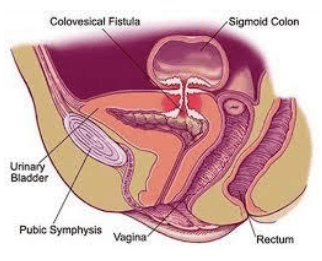
Hình 6: Rò đại tràng – bàng quang
3.4. Anal fisting
Fistula between the anal canal and the skin around the anus. Usually develops from an anal abscess that ruptures and expels the contents of the abscess to the skin. anorectal abscesses are more common in men, especially gay men. The patient presented with severe perineal pain, recurrent abscesses, and fever. Careful examination of the perineal areas or rectal examination should be performed for fistulas.
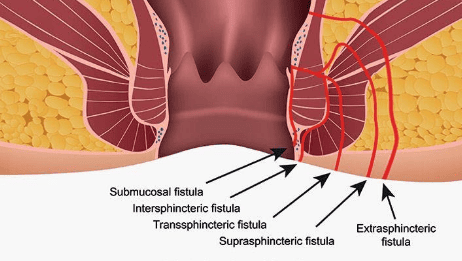
Hình 7: Bệnh lý rò hậu môn

Hình 8: Một bệnh nhân bị rò hậu môn
Anal fistula, the most effective treatment today is fibrous fistula removal. Although there are some cases of complicated fistula, difficult to treat, but in general this type of gastrointestinal fistula has the best prognosis.
4. Classification of gastrointestinal fistulas according to leak volume
Low-volume leak less than 200ml/24 hours, moderate-volume leak from 200-500ml/24 hours, and high-output leak above 500ml/24 hours. Although spontaneous healing rate is not clearly related to fistula output, moderate and high volume fistulas are often associated with small bowel fistulas.
5. Causes of Gastrointestinal Leaks
Quite complicated, 75 to 85% of cases are complications after surgery. The remaining 15-25% of cases are spontaneous fistulas. Gastrointestinal fistula after surgery depends on many factors such as the pathological condition and the anatomical and physiological structure of the organs.
The surgeries that are more likely to cause fistulas are inflammatory bowel diseases, cancer, or bowel dissection. In particular, diseases such as cancer of the esophagus, rectum, and pancreatic head have a higher rate of postoperative anastomosis than diseases of the stomach and small intestine due to their own anatomical, physiological and pathological characteristics. . Emergency surgery such as pancreaticoduodenectomy, the rate of gastrointestinal fistulae after surgery is often high, and due to the anatomical structure of the duodenal frame, there is always great pressure because of the amount of secretions from the stomach, duodenum, bile, and fluid. pancreatitis and the activation of pancreatic enzymes, especially when the patient is managed late after 24 hours in the presence of peritonitis. The above complications often occur when the patient is not well prepared, has emergency surgery, or the patient has received radiation therapy before, the elderly patient has cardiopulmonary diseases, chronic diabetes. Poor nutritional status plays a major role in the failure of the gastrointestinal tract to heal and the body's inadequate response to post-operative inflammation.
In addition, surgical techniques, sutures and experience of surgeons and tools such as needles and surgical sutures play an important role in wound healing as well as gastrointestinal complications.
People with Crohn's disease: Colectomy surgery or anastomosis of the colon and small intestine on Crohn's disease patients will easily lead to anastomosis and gastrointestinal fistula, because the tissue in the anastomosis is no longer intact. normal. Even appendectomy in patients with Crohn's disease can lead to gastrointestinal fistulae.
6. Causes of complications and death in gastrointestinal tract
Three classic complications are common in gastrointestinal fistula: electrolyte disturbances, malnutrition, and infection. The frequency of these complications is directly related to the output of the probe. Although spontaneous healing rate is not clearly related to fistula output, moderate and high volume fistulas are often associated with small bowel fistulas.
Electrolyte disturbances (defined within 48 hours) determined by monitoring of arterial blood gases and plasma electrolyte concentrations. Commonly disturbed electrolytes are Sodium, Potassium, Magnesium and Phosphate in cases of complete parenteral nutrition.
Malnutrition is often associated with leaky output. Infection and malnutrition are common in high-output fistulas. Clearly, when the infection is not controlled, even providing adequate nutrition will not improve malnutrition. Once the infection has been controlled, ie closed foci of infection (abscess) may have formed, it is necessary to continue to have a CT scan or an MRI to confirm it. These abscesses need to be drained to resolve the infection. Surgical surveillance, total bowel debonding, reestablishment of circulation and drainage of abscesses, this surgery called “reconstruction of function” by Welch, was originally intended to reestablish circulation. digestion and absorption of nutrients. But now that nutrition can be delivered in many ways, the aim of the surgery is to re-establish circulation and drain the abscess.
7. Diagnosis of gastrointestinal fistula
Role of Contrast Fistula and Fistula: Enterocutaneous fistula can be fully described with fistulography in most cases. In some cases, the probe line may be better visualized with the use of contrast medium. The most common method for fistula radiography is to insert a flexible catheter and inject a water-soluble contrast agent into the fistula, with fluoroscopy guidance. show intestinal anastomosis and any abscesses if involved, whereas CT is often performed adjunctively, not only to help identify all abscess cavities but also to guide percutaneous drainage Fistula MRI: With the advent of modern MRI machines, which have made the fistula assessment more accurate, the advantage of MRI is that it is a better soft tissue assessment than CT Scan in most cases.
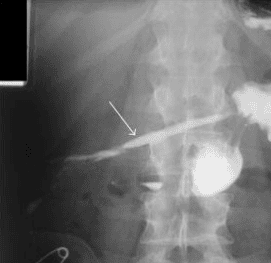
Hình: Dò dạ dày ra da sau mổ thủng dạ dày, hình mũi tên màu trắng chỉ vị trí thuốc cản quang chảy từ dạ dày ra thành bụng
In addition, hydrogen peroxide-enhanced ultrasound has been used recently in several centers to delineate enterocutaneous fistulas.
Gastrointestinal endoscopy plays an important role in the diagnosis of gastrointestinal fistula. This method has both determined the location of the fistula, the size of the fistula, and the prognosis for surgery. Through endoscopy, it is possible to intervene to block the fistula with specialized tools.
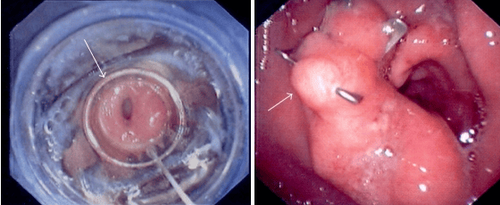
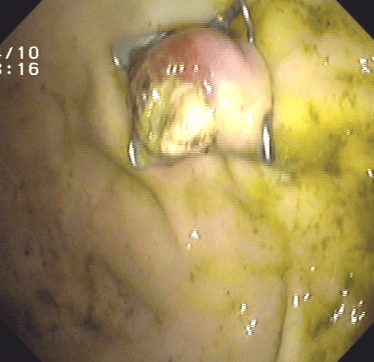
Hình 9: Lỗ dò dạ dày ra ổ bụng sau mổ thủng dạ dày. Sau đó lỗ dò được đóng lại thành công bằng dụng cụ Over The Scope Clip (OTSC)
8. Treatment of gastrointestinal fistula
Depends largely on the cause and extent of the fistula. Assess the patient's condition, give aggressive medical treatment so that the fistula can heal naturally. Conservative medical management is the initial standard approach for postoperative enterocutaneous fistulas. Other supportive measures include appropriate antibiotic regimens and electrolyte balance. Surgical interventions are indicated when conservative measures are unsuccessful or there are signs of peritonitis.
In the 1960s, postoperative gastrointestinal fistulas often had serious complications and high mortality. The point of view at this stage is early surgery to restore gastrointestinal circulation in the hope of resolving the patient's early infection and malnutrition. However, this strategy has not been successful because the failure rate is too high up to 80% of cases with early intervention. Mortality rates reach 40 to 60%. In the later period, with a deeper understanding of the pathophysiology and nutrition, along with the advent of more powerful antibiotics and better nutrients, conservative treatment has reduced mortality. and gastrointestinal complications. Surgery is only indicated when conservative treatment fails. The timing of surgical intervention is also considered to suit each type of surgery. The most important issue is to ensure that nutrition and infection control before surgery are at an acceptable level. Many authors recommend surgery if conservative treatment fails after 4 to 6 weeks. Antibiotics and nutrition are only effective when the abscess is well drained. It is recommended to use antibiotics that can penetrate into the abscess well such as: Dalacin C, ... Invanz. However, surgery still has certain limitations such as: surgery on patients with poor nutrition, prone to perioperative infection, much sticky tissue around the fistula, difficult to remove...
Today, with Advances in flexible gastrointestinal endoscopy have contributed to the success of the treatment of gastrointestinal fistulas. One of the techniques used to treat gastroenteritis is the Over-the-scope clip (OTSC). This is a new type of clip that is very useful not only for suturing holes and fistulas but also very useful in endoscopic hemostasis. The advantage of the over-the-scope clip (OTSC) is that the operation is simple and quick, similar to elastic band ligation of the esophageal varices, and at the same time, this clip adheres very tightly to the wall of the digestive tract...
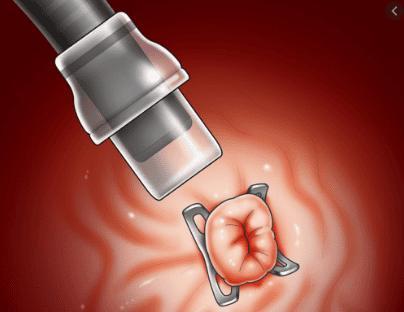
Hình 10: Dụng cụ OTSC kẹp lỗ dò
Hình 11: Lỗ dò dạ dày ra da được khép thành công với dụng cụ OTSC
Diagnosis and treatment of gastrointestinal fistulas is still a major diagnostic challenge today. Knowledge of the different types of gastrointestinal fistulas and their causes is important for proper patient care. With the advancement of science, there are more and more less invasive intervention methods to treat this disease, improving the quality of life for patients.
Gastrointestinal cancer screening is a scientific and effective measure to detect gastrointestinal cancer early (esophageal cancer, stomach cancer, colon cancer) and provide a good treatment plan. best. Currently, Vinmec International General Hospital has a package of screening and early detection of cancers of the gastrointestinal tract (esophagus - stomach - colon) combined with clinical and paraclinical examination to bring the most accurate results. maybe.
When screened for gastrointestinal cancer at Vinmec, you will receive:
Gastrointestinal specialty examination with an oncologist (by appointment). Gastroscopy and colonoscopy with an NBI endoscope with anesthesia. Peripheral blood cell total analysis (by laser counter). Automated prothrombin time test. Automated thrombin time test. Activated Partial Thromboplastin Time (APTT) test using an automated machine. General abdominal ultrasound To register for screening and treatment of gastrointestinal diseases at Vinmec International General Hospital, you can contact Vinmec Health System nationwide, or register for an online examination.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.