This is an automatically translated article.
Posted by Doctor Mai Vien Phuong - Department of Medical Examination & Internal Medicine - Vinmec Central Park International General Hospital
Lymphoma occurs in many organs of the body, but there is a lymphoma involving the gastric mucosa caused by Helicobacter Pylori, which has received little attention, which will be discussed in this article.
Welcome to read : Gastric maltoma Part 1: Overview, diagnosis and symptoms
1. Anatomy of MALT . tumor
The lesion morphology described by Issacson and Wright includes:
Long-term disease course with progressive chronic mucositis Tend to diffuse and destroy epithelial morphology, such lesions are called “epithelial infiltrates” Lymphoepithelial MALT lymphocytes have a "homing" appearance with typical diffuse multifocal lesions. Gastric MALT lymphoma does not have a specific immune marker, but it is positive for markers: CD19, CD 20, CD 22, CD 79a, negative for CD 10, CD 5, Cyclin D1 to help differentiate from follicular lymphoma and Mantle cells. More than 90% of gastric lymphomas are equally divided into two histological types[11]: MALT lymphoma: rate 38-48%, Diffuse large B-cell lymphoma: incidence 45-59%; The remaining cases of gastric lymphoma may represent any lymphoid histology, but the most commonly seen are: Mantle cell lymphoma: 1%, Follicular lymphoma: 0.5 - 2%, Extracellular T-cell lymphoma margin: 1.5 - 4%.
2. The role of gastrointestinal endoscopy
Endoscopic examination with biopsy and histopathology is a standard practice in the diagnosis of gastric MALT lymphoma. HP-negative gastric MALT lymphoma lesions were similar to those observed in HP-positive subjects[13].
In addition to histopathology, immunohistochemistry for B-cell markers can aid in the diagnosis. Macroscopic gastric mucosal changes that are nonspecific include: thickening of mucosal folds, irregular hemorrhagic nodules, lymphomatous polyposis, edema, warts, and ulcers. The distribution of the lesions is often patchy, with multiple sites. Therefore, multi-site biopsies are recommended during endoscopic examination of the stomach, and that an adequate number of biopsies should be performed from the lesion both to make an accurate diagnosis and to rule out the possibility of a diagnosis. In the presence of diffuse large B-cell lymphoma, Fischbach suggested that at least ten biopsies be required.
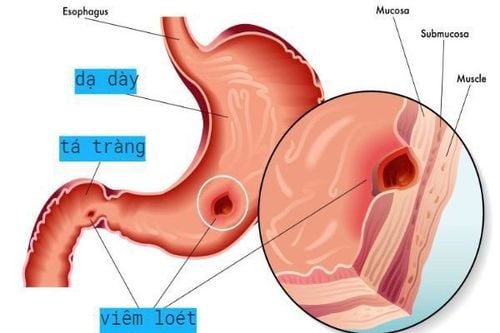
Many gastric MALT lymphoma lesions are similar to early gastric cancer, gastritis, or peptic ulcer, but distinguishing between the two groups is important because the treatment for these conditions is different.

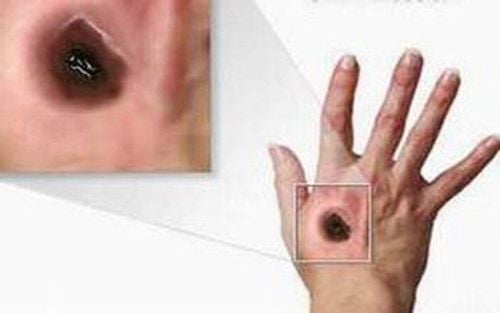
Hình 6: Tổn thương dạng loét ở dạ dày, kết quả mô bệnh học là U MALT

Hình 7: Một số hình ảnh u MALT dạ dày, rất dễ bỏ sót nếu không khảo sát kĩ dạ dày. Nguồn ảnh: semanticscholar.org

Hình 8: Hình ảnh nội soi và mô học của U MALT. Nguồn ảnh: semanticscholar.org
3. MALT . tumor staging
Endoscopic ultrasound is used to determine gastric wall infiltration, regional lymph node involvement and it is also used in remission monitoring.
Adjusted Ann Arbor grade for gastric MALT lymphoma:
Stage I: Tumor confined to stomach (mucosa, submucosa, muscle). Stage II: Invasive tumor, infiltrating lymph nodes. II1: Perigastric lymph node infiltration. II2: Distal lymph node infiltrates (America - vena cava, iliac vein ..). IIE: Invasion through the serosa to surrounding organs or tissues. Stage IV: Diffuse intra-abdominal lymph node infiltrates, supradiaphragmatic lymph node infiltrates.

Hình 9: Một trường hợp U MALT được đánh giá giai đoạn qua siêu âm nội soi Nguồn ảnh: researchgate.net
4. Treatment of MALT . tumors
HP eradication therapy has become the first-line therapy in the treatment of gastric MALT lymphoma accepted in the US National Cancer Network (NCCN) and European Cancer Society (ESMO) guidelines. ). Numerous studies have highlighted the complete histopathological response to HP eradication, remission in up to 80% of patients without additional treatment. The time required to obtain a histopathological response can range from several months to more than a year. Standard triple antibiotic therapy includes a combination of amoxicillin, clarithromycin, and a PPI. In Vietnam, due to the increasing resistance of HP, alternative treatment is suggested, such as using metronidazole instead of clarithromycin. In up to 20% of patients who require a second HP eradication regimen with an alternative three- or four-drug regimen prior to other treatment options, second-line therapy should be instituted.
Treatment options after failure to eliminate HP include observation, radiation therapy, surgery, chemotherapy, monoclonal antibody therapy. Surgery no longer plays an important role in the treatment of gastric MALT lymphoma, with the exception of rare complications such as bleeding, pyloric stenosis, or perforation that cannot be controlled endoscopically.
For H-negative gastric MALT lymphoma or in patients unresponsive to antibiotic therapy, 30Gy radiotherapy, including the stomach and perigastric lymph nodes, has been accepted as a modality of treatment. topical treatment. Several retrospective studies have reported that radiation therapy has excellent outcomes, 93-100% response, and minimal toxicity in patients with gastric MALT lymphoma. Chemotherapy and the monoclonal antibody Rituximab can be used in all stages of the disease or a combination of both. The combination of rituximab (CD20 positive cases) improves disease response and survival, for patients with invasive tumor, histopathologic transformation, or an unfavorable prognostic score, one Anthracycline combination regimens should be used. Bendamustine is a good choice for young patients diagnosed with MALT lymphoma.
5. Prognosis of MALT . tumor
Prognosis MALT gastric lymphoma is considered a cancer with good prognosis, tends to remain in situ for a long time rather than metastasize, In early stage, low risk factor 5 progression-free survival, overall survival was 76% and 99%, respectively. Gene mutation is also an interesting factor in the prognosis of gastric MALT lymphoma. Mutation (11,18) is a predictor of failure to respond to HP eradication therapy in all stages of gastric MALT lymphoma.
6. Conclusion
Gastric MALT lymphoma is a rare disease associated with HP infection. The disease responds completely to antibiotic therapy that eradicates HP in the early stages. Most cases of gastric MALT lymphoma are cured with HP eradication therapy, but there are cases where chemotherapy and radiation therapy are required. It is essential to have appropriate endoscopic follow-up and follow-up for histological regression, to prevent histological changes and widespread progression. Radiation therapy is the modality used in gastric MALT lymphoma when the lesion is localized.Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
We invite you to follow-up Gastric ulcer Part 1: Overview, diagnosis and symptoms
References:
Asano N, Iijima K, Koike T, Imatani A, Shimosegawa T. Helicobacter pylori-negative gastric mucosa- associated lymphoid tissue lymphomas: A review. World J Gastroenterol. 2015. Ye H, Liu H, Raderer M, et al. gastric MALT lymphoma Brief report High incidence of t (11;18) (q21;q21) in Helicobacter pylori – negative gastric MALT lymphoma. 2013. Koch P, del Valle F, Berdel WE, et al. Primary gastrointestinal non-Hodgkin's lymphoma: I. Anatomic and histologic distribution, clinical features, and survival data of 371 patients registered in the German Multicenter Study GIT NHL 01/92. J Clin Oncol. 2001;19(18):3861- 3873. doi:10.1200/JCO.2001.19.18.3861 Ruskone-Fourmestraux A, Lavergne A, Aegerter PH, et al. Predictive factors for regression of gastric MALT lymphoma after anti-Helicobacter pylori treatment. Gut. 2001;48(3):297-303. doi:10.1136/gut.48.3.297