This is an automatically translated article.
The article was professionally consulted by an Anesthesiologist - General Surgery Department - Vinmec Nha Trang International General Hospital.A complete hysterectomy is performed when the patient has severe uterine disease for which other treatments have not been effective. Epidural anesthesia is the anesthetic method used in many cases of total hysterectomy.
1. What is a total hysterectomy?
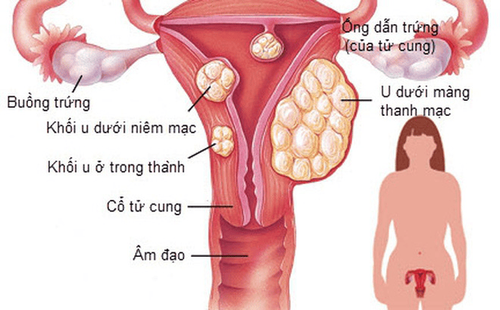
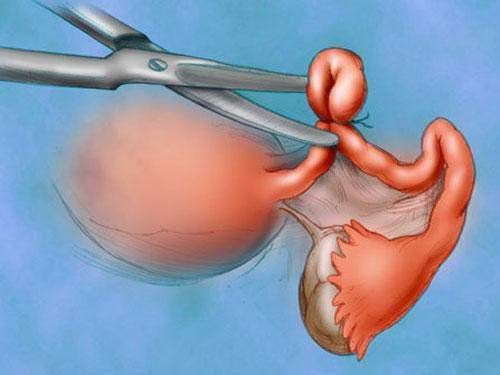
Total hysterectomy is performed when the patient has serious uterine diseases such as uterine cancer, cervical cancer, uterine fibroids, endometriosis, etc. Other treatments are not effective. If the uterus is not removed, it will greatly affect health, even endanger the patient's life. During a hysterectomy, the doctor removes the entire uterine mass including the cervix and the body of the uterus. Once the uterus is removed, the woman will no longer be able to reproduce, so when a complete hysterectomy is indicated, the doctor must carefully weigh the benefits and risks, and perform surgery. Surgery is performed only with the consent of the patient or the patient's family.In order to perform surgery, anesthesia is an extremely important step. A good anesthetic method will help patients reduce anxiety, painless during surgery, help soft muscles for convenient surgery while still ensuring patient safety. Epidural anesthesia is an anesthetic method used in many cases of total hysterectomy. Anesthesia will be injected into the epidural space of the patient to temporarily inhibit segmental nerve conduction through the nerve roots for the purpose of analgesia during hysterectomy and pain relief after hysterectomy. bow .

Phẫu thuật cắt tử cung hoàn toàn được thực hiện khi người bệnh mắc các bệnh lý nặng vùng tử cung
2. Complete hysterectomy with epidural anesthesia
2.1. Indications and contraindications Epidural anesthesia is indicated as an anesthetic method for hysterectomy when the patient has no contraindications to anesthesia. Epidural anesthesia is also used to relieve pain after surgery.Epidural anesthesia is not performed in the following cases:
The patient refuses to perform the method. The patient is allergic to the anesthetic, has an infection in the needle puncture area. coagulopathy or inadequate discontinuation of anticoagulants. Patients with constricted mitral stenosis, constricted aortic valve, severe decompensated heart failure. 2.2. Preparation for performing epidural anesthesia in a total hysterectomy The epidural will be administered by a specialist anesthesiologist. Necessary anesthetic and anesthetic facilities and equipment include:
Needle needles of all sizes, gloves, sterile gauze, pince, antiseptic alcohol, sterile hole towels,... Epidural anesthesia kits Hard local anesthetics: lidocaine, bupivacaine, levobupivacaine, ropivacaine,... can be combined with drugs of the morphine, adrenaline, clonidine family,... Dosage will be calculated by the doctor based on weight, height and body type. patient status. In addition, to ensure safety during anesthesia and surgery, emergency and monitoring facilities are required, including:
Resuscitation facilities: Oxygen source, Ambu balloon, mask, internal intubation equipment tracheostomy, electric shock machine, anesthesia machine with breathing, suction machine,... And the means of routine monitoring of electrocardiographic indicators, blood pressure, oxygen saturation, breathing rate,... Weekly resuscitation drugs complete solution including intravenous fluids, adrenaline, ephedrine,... Anticonvulsants such as barbituric drugs, benzodiazepines, muscle relaxants, Intralipid 20%,... On the patient's side, to prepare for anesthesia before surgery , the doctor will examine before surgery, explain to the patient the purpose of anesthesia so that the patient cooperates when performing. The anesthetic area will be kept clean. In some necessary cases, the patient will be given sedation the night before surgery.

Trong một số trường hợp, bệnh nhân sẽ được cho sử dụng thuốc an thần vào tối trước hôm mổ
Sitting position: The patient sits with his back arched, head bowed, chin resting on chest, legs stretched out on face operating table or feet resting on the chair. Or lying position: The patient lies on his side, back arched, knees close to the abdomen, chin resting on the chest. The doctor performing anesthesia will wear a hat, mask, wash hands, wear a shirt, and wear sterile gloves. Disinfect the puncture site three times with an antiseptic solution, then cover with a sterile tissue. Apply local anesthesia with Lidocaine 1-2%.
The epidural steps for a complete hysterectomy include:
Midline or lateral anesthesia can be chosen. If anesthesia is applied to the midline, the doctor will insert a needle into the space between the two posterior spines, the puncture location will depend on the high or low surgical position. If anesthesia is applied to the lateral line, proceed to insert the needle 1-2cm from the midline, directing the needle in the middle, up, and forward. The epidural space is identified by findings such as spinal ultrasonography or methods of loss of resistance, hanging drops. The needle is in the correct position when resistance is lost and there is no regurgitation of cerebrospinal fluid and blood. With the needle bevel facing up, insert the catheter slowly with a length of 3-5cm in the epidural space. Withdraw needle Tuohy. Test and test with 2-3ml lidocaine 2% mixed with adrenaline 1/200.000. Secure the catheter with a sterile bandage. The drugs that can be used for epidural anesthesia are: lidocaine 2% 300-400mg; ropivacaine 0% 75-125mg; bupivacaine 0.5% 75-125 mg; levobupivacaine 0.5% 75-125mg. In addition, combination drugs can be used: morphine 2-4mg; sufentanil 10-20mcg not to exceed 30mcg/kg; fentanyl 50-100mcg. To relieve pain after hysterectomy, conduct continuous infusion of bupivacaine 0.1 - 0.125 at a speed of 4-6ml/hour, ropivacaine 0.08 - 0.125 at a rate of 4-10ml/hour; levobupivacaine 0.125 rate 4-10ml/hour. Concentrations of combination drugs are: morphine 10-20mcg/ml; fentanyl 1-2mcg/ml; sufentanil 0.5 mcg/ml.
3. Possible complications with epidural anesthesia for complete hysterectomy and how to handle

Đau đầu là một trong số những phản ứng có thể gặp phải sau khi thực hiện kỹ thuật vô cảm
If the patient has signs of allergy, anaphylaxis with local anesthetics. The doctor will immediately stop the drug and start an anti-anaphylactic regimen. If the patient is poisoned by local anesthetics due to the wrong injection into the blood vessels (or the drug is absorbed too quickly, or because of the body...). The doctor will immediately stop the drug, perform respiratory and circulatory resuscitation, anticonvulsant and use specific drugs to help neutralize the effect of the anesthetic. 3.2. Complications due to epidural technique and management
Epidural Perforation: If this is the case, the anesthesiologist will withdraw the needle and move the needle to another puncture site (above the old one) or switch to another anesthetic method. . General spinal anesthesia by injecting anesthetic into the subarachnoid space: Perform respiratory and circulatory resuscitation emergency for the patient. Patients with low blood pressure, slow pulse: The doctor will treat with vasoconstrictor drugs (such as phenylephdrine, ephedrine, adrenalin,...), atropin and fluid rehydration. Patients with headache after anesthesia: The doctor will make the patient lie down, give enough fluids, use painkillers and patch the dura with autologous blood (Blood patch) if other measures are not effective after 24 hours. Patients with nausea and vomiting: Control blood pressure and use antiemetics for patients. Patients with urinary retention: Apply warm compresses and catheterize the patient's bladder if necessary. In addition, other possible complications of epidural anesthesia are epidural hematoma, nerve root damage, meningitis, cauda equine syndrome, epidural abscess,... Depending on the situation When encountering situations, doctors will conduct consultations and explorations to have appropriate treatment. If the epidural fails, the anesthetic team will switch to another method of anesthesia.
Vinmec International General Hospital with a system of modern facilities, medical equipment and a team of experts and doctors with many years of experience in medical examination and treatment, patients can rest assured to visit. examination and treatment at the Hospital.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.