This is an automatically translated article.
The article is professionally consulted by Specialist Doctor I Nguyen Thanh Hai - Radiologist - Department of Diagnostic Imaging and Nuclear Medicine - Vinmec Times City International Hospital
Intestinal obstruction is a blockage of circulation in the intestinal lumen that prevents food or liquid from passing through the small intestine or large intestine (colon). Common causes of bowel obstruction include bands of fibrous (adhesive) tissue in the abdomen that form after surgery, inflamed intestines (Crohn's disease), complicated diverticulitis, hernias, and colon cancer. If not treated properly and promptly, it can lead to dangerous complications (intestinal necrosis, peritonitis, infection-toxicity). To diagnose intestinal obstruction, doctors need to combine clinical examination with imaging methods such as abdominal X-ray, ultrasound, abdominal CT scan and other laboratory tests to provide information needed for diagnosis.
1. What is an intestinal obstruction?
Intestinal obstruction or gastrointestinal obstruction is a condition in which the digestive tract is blocked. The digestive tract includes the esophagus, stomach, small intestine, and large intestine. Common symptoms of intestinal obstruction:
Abdominal pain intermittently, pain relief after passing, defecation. Secrets, defecation. Nausea, vomiting. Discomfort in the abdomen. Constipation . Loss of appetite, loss of appetite.

Tắc ruột hay tắc nghẽn đường tiêu hóa là tình trạng ống tiêu hóa bị bít tắc.
2. Causes of bowel obstruction
2.1. Causes of Intestinal Obstruction Here are some easy causes of bowel obstruction:
Inflammatory bowel disease: Crohn's, tuberculosis... Intestinal tumor. Intussusception, intestinal volvulus. Inflammation of the small intestine caused by radiation therapy in cancer treatment. Hematoma in the intestinal wall (due to anticoagulation therapy, or trauma). 2.2. Causes of Extraintestinal Obstruction Adhesions are the main cause of intestinal obstruction, mainly occurring after surgery, accounting for 50%-80% of cases, a few are due to peritonitis. Hernia: The second most common cause of intestinal obstruction, accounting for 10% of cases. 2.3. Intraluminal causes of obstruction Gallstone ileus is a rare complication that results in migration of large gallstones through the biliary fistula and intestine. Gastric foreign body: Rare, but the number is increasing due to the increasing frequency of gastric bypass surgery. Food residue, worm tufts.
Bệnh viêm ruột: Crohn là một trong những nguyên nhân gây tắc ruột.
3. Diagnosis of intestinal obstruction
The doctor will examine your abdomen and ask you about the symptoms you are experiencing. They also review medical history and current medications. When they suspect you have a bowel obstruction, your doctors will ask you to do some more laboratory tests that will help you make a final diagnosis. Tests to do:
X-ray - X-ray. Supersonic. CT - Scanner.
4. Is X-ray or ultrasound valuable in diagnosing bowel obstruction?
Currently, due to the development of medical technology, many advanced abdominal imaging tools are used in medical facilities for the subclinical diagnosis of intestinal obstruction.
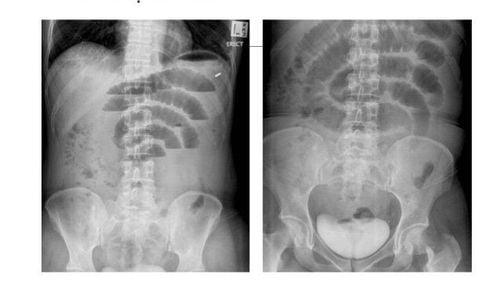
Routine abdominal X-ray is still the first used imaging modality for patients with bowel obstruction. Although, X-ray is always available in medical facilities and relatively low cost, but X-ray method only allows specialists to diagnose 50% - 60% of bowel obstruction cases. to a severe degree. As recommended by experts, the results of this approach should be used as a basis for the classification of bowel obstruction, and to aid in treatment decisions.
Ultrasonography is not widely used in the evaluation of bowel obstruction because of a number of reasons, mainly because the abdominal loops of flatulence and adhesions are not detected by this technique. Currently, methods of increasing contrast with contrast agents to evaluate the intestinal wall such as small bowel contrast enema (enteroclysis) are evaluated as highly accurate diagnostic methods in cases of intestinal obstruction.
Routine CT is the dominant imaging modality for preoperative evaluation of intestinal obstruction, with sensitivity of 90%-96%, specificity of 96%, and accuracy of 95%. Multi-probe CT scanners have the ability to reconstruct multiple planes to make the diagnosis more effective in the evaluation of bowel obstruction. Because CT has the potential to detect dangerous complications such as intestinal ischemia, bowel necrosis, intestinal perforation, and peritonitis, it should be considered the best means of determining which patients benefit if conservative treatment and close follow-up, which patients benefit from immediate surgical treatment.

Chụp X-Quang bụng thường quy vẫn là phương pháp chẩn đoán hình ảnh được sử dụng đầu tiên cho các bệnh nhân tắc ruột.
4.1. X-ray film of the abdomen
One of the difficulties for surgeons and radiologists when diagnosing patients with suspected bowel obstruction is deciding which imaging technique to use first (based on the patient's symptoms and presentation). ) to identify bowel obstruction and help make the best treatment decision for the patient in a timely manner.
Routine abdominal X-ray is preferred as the first imaging modality. The results of this technique are diagnostic in 50%-60% of cases; unclear in 20-30%; normal, unspecified, or misleading in 10%-20%. The images and values on the abdominal X-ray are indicative of clear bowel obstruction, and if clinical bowel obstruction is severe or complete, the patient should be referred to surgery immediately. However, if immediate surgery is not planned or other treatment options are considered, specialists should prioritize assessment of severity and cause with computed tomography (CT) imaging. scan).
In contrast, if the initial radiographic findings are normal, equivocal, or suggestive of partial bowel obstruction, then the patient should maintain close communication between the surgeon and the physician. radiologist to ensure appropriate clinical and radiological follow-up.
Although the diagnostic accuracy and specificity of abdominal radiographs are low, detecting clear bowel obstruction in suitable laboratory patients is of great value and contributes greatly to the initial diagnosis. and decide on treatment.
Therefore, the parameters and images on the X-ray film to diagnose intestinal obstruction allow the specialist to distinguish between the large and the small bowel obstruction in terms of diameter and dilatation of the colon loops. the largest, and the number of elastic bands more or less. In the experience of some gastrointestinal radiology specialists, there are several other significant and predictive signs of severe bowel obstruction that are more than two air-fluid levels. legs wider than 2.5cm and air-fluid levels in the same loop with legs more than 2cm apart in height.

Những thông số và hình ảnh trên phim X-Quang chẩn đoán tắc ruột cho phép các bác sĩ chuyên khoa chẩn đoán phân biệt giữa tắc ruột mức độ nhiều và mức độ ít.
4.2. Signs on ultrasound
In the US, ultrasound is not the first choice used for the initial assessment of bowel obstruction. However, ultrasound is routinely used in countries where CT is not common and where ultrasound experience is high. Although the technique is operator dependent and there are limitations when evaluating structures. Some causes of bowel obstruction such as foreign bodies, intussusception, Crohn's disease and tumors can be detected by ultrasound.
Ultrasound has an important role in assessing the severity of intestinal obstruction. When present between the loops of dilated bowel, without peristalsis, wall thickening (>3 mm) in the dilated small intestine is filled with fluid suggestive of intestinal infarction.
Finally, it is important that before a patient with bowel obstruction, the physician will consider the symptoms and recommend the necessary tests to make a diagnosis. Combining imaging methods: abdominal x-ray, abdominal ultrasound, and CT scan will provide important information to help make an accurate diagnosis for timely treatment of intestinal obstruction, limiting serious complications that cause serious complications. severe consequences for the patient.
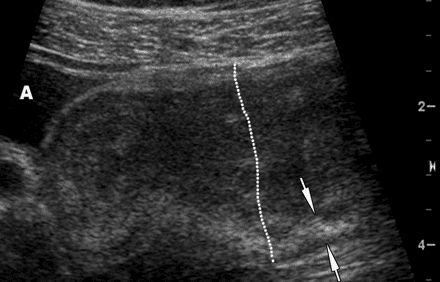
Siêu âm có vai trò quan trọng trong việc đánh giá mức độ trầm trọng của tắc ruột.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.