This is an automatically translated article.
Posted by Master, Doctor Mai Vien Phuong - Department of Examination & Internal Medicine - Vinmec Central Park International General Hospital
The diagnosis of GERD is difficult and is often made with a combination of clinical symptoms, response to acid suppression, as well as objective examination with upper gastrointestinal endoscopy and esophageal pH monitoring.
6. 24 hour esophageal pH measurement
Ambulatory reflux monitoring (24-hour esophageal pH measurement) is the only method that allows direct measurement of esophageal acid exposure (acid exposure time, acid exposure time), frequency Reflux episodes and the relationship between symptoms and episodes of reflux. It is often used to evaluate patients with no endoscopic evidence of GERD, to confirm the diagnosis. It can also be used to monitor reflux control in people undergoing treatment with persistent symptoms.
24-hour esophageal pH measurement allows monitoring of the presence of acid in the esophagus to be recorded for 24 hours with a nasal pH catheter placed near the lower esophagus. When there is movement of stomach acid into the esophagus during reflux, it lowers the pH of the esophagus. The test is considered positive if the pH drops below 4 for longer than 5 seconds. Tracking of patients is analyzed and results are expressed using six standard components. Of these 6 parameters, a pH score known as the DeMeester Score was calculated, which is a global measure of esophageal acid exposure.
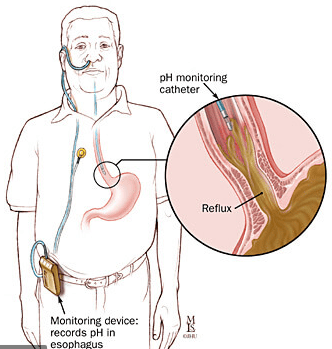
Dụng cụ đo pH thực quản 24 giờ
There are limitations with the use of 24h pH measurement to diagnose GERD. The frequency of symptoms may vary. It is unlikely that symptoms will occur during a routine 24-hour follow-up session and therefore a single measurement may not be representative. In addition, pH monitoring cannot diagnose non-acid reflux (pH > 4)
24 h esophageal pH impedance monitoring is a technique used in the diagnosis of GERD, by monitoring both impedance and pH. An impedance pH probe is inserted into the nostril and into the esophagus. The impedance pH probe will stay in place for 24 hours and is connected to a small recorder.
7. Gastrin 17
Gastrin 17 (G-17) is a gastrointestinal peptide hormone and is involved in the control of gastric acid secretion. It is secreted almost exclusively by G antral cells. G-17 controls gastric acid secretion by a negative feedback mechanism. G cells are stimulated by high gastric pH. High acidity in the stomach inhibits G-17 secretion. Thus, gastrin levels indirectly reflect the acidity of the stomach.

Vai trò của G-17 trong việc kiểm soát tiết axit dạ dày
Franceschi et al. evaluated the role of Gastropanel® (Biohit Oji, Finland), a noninvasive serological test, in the screening of chronic atrophic gastritis in a dyspeptic population. In this population, individuals with GERD showed significantly lower G-17 levels than other patient groups. Goni and associates. confirmed the measurement results and determined that a G-17 value <1.9 pmol/L was useful for the diagnosis of GERD.
The role of G-17 in the diagnosis of GERD was assessed by measuring pH and pH impedance in two different studies. In both studies, it can be concluded that G-17 seems to be able to identify patients with GERD and assess the nature of reflux.
Low G-17 levels are useful to identify not only patients with typical symptoms but also those with atypical manifestations of GERD.
Therefore, his serum G-17 level is suggested as a promising and useful first-degree test for diagnosing GERD even in the presence of atypical presentation.
GastroPanel® Gastrin-17 is an enzyme-linked immunosorbent assay (ELISA) for the quantitative measurement of gastrin-17 (G-17) in human EDTA plasma samples.
Conclusion
GERD is a complex disease with heterogeneous symptoms and a multifaceted etiology that challenges a simple diagnostic algorithm or classification by classification.
Ambulatory esophageal pH monitoring helps identify GERD in patients with persistent symptoms (both typical and atypical) in the absence of esophageal mucosal injury, especially especially when the acid suppression test fails.
New metrics from pH impedance monitoring, mean basal impedance index nocturnal index, and peristaltic wave index due to reflux swallowing, can differentiate GERD from No-GERD patients and predict PPI response .
Future studies are warranted to confirm the value of Gastrin-17 as a noninvasive marker for the diagnosis of GERD, both in patients with typical and atypical symptoms.
Vinmec International General Hospital examines and treats gastroesophageal reflux disease with the most optimal internal - surgical methods for patients, both children and adults. Coming to Vinmec International General Hospital, patients will receive a direct, dedicated and professional examination from a team of qualified and experienced medical staff.
If you have a need for consultation and examination at Vinmec Hospitals under the nationwide health system, please book an appointment on the website for service.
Please dial HOTLINE for more information or register for an appointment HERE. Download MyVinmec app to make appointments faster and to manage your bookings easily.
ReferencesCesario Silvia,1 Scida Serena, et al., Diagnosis of GERD in typical and atypical expressions, Acta Biomed. 2018; 89(Suppl 8): 33–39. El-Serag Hashem B, et al. “Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review” Gut. 2013 gutjnl-2012. [PMC free article] [PubMed] [Google Scholar] Vakil Nimish, et al. “The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus” The American journal of gastroenterology. 2006;101(8):1900. [PubMed] [Google Scholar]4. Vaezi Michael F. “Atypical expressions of gastroesophageal reflux disease” Medscape General Medicine. 2005;7(4):25. [PMC free article] [PubMed] [Google Scholar]5. Lacy Brian E, et al. “The diagnosis of gastroesophageal reflux disease” The American journal of medicine. 2010;123(7):583–592. [PubMed] [Google Scholar]6. Aanen M. C, et al. “Diagnostic value of the proton pump inhibitor test for gastro-oesophageal reflux disease in primary care” Alimentary pharmacology & therapeutics. 2006;24(9):13771384. [PubMed] [Google Scholar]